

Noninvasive Ventilation Use in Critically Ill Patients with Acute Asthma Exacerbations
- PMID: 32663410
- PMCID: PMC7706169
- DOI: 10.1164/rccm.201910-2021OC
Noninvasive Ventilation Use in Critically Ill Patients with Acute Asthma Exacerbations
Abstract
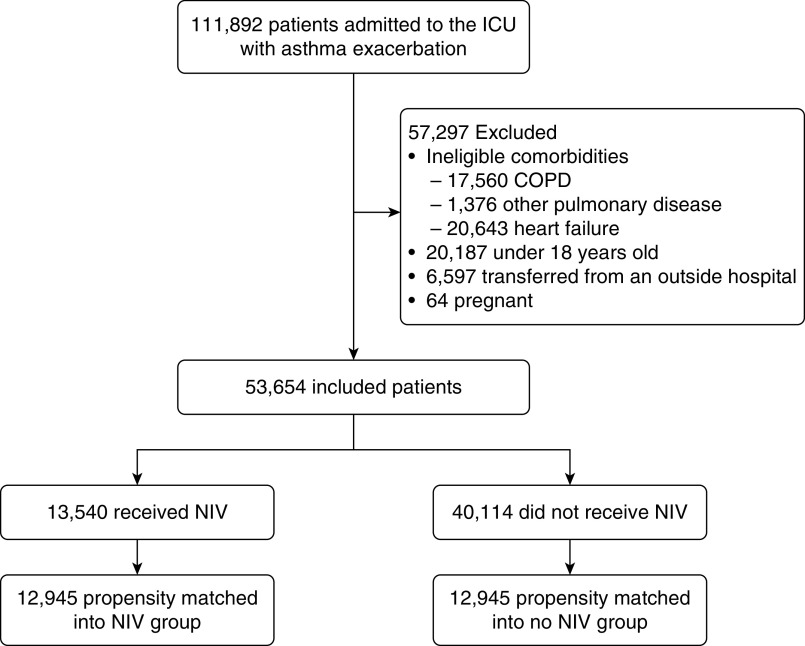
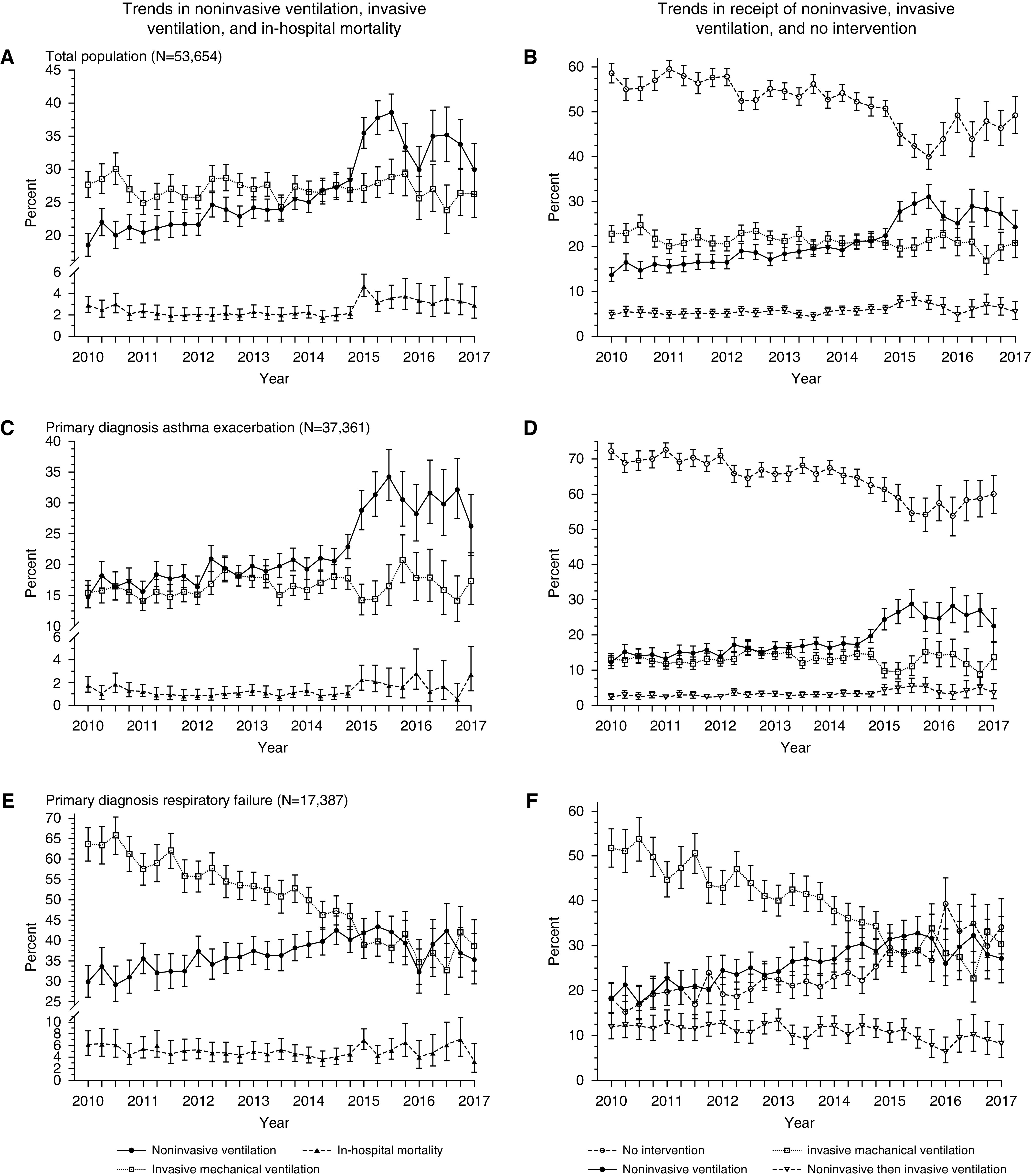
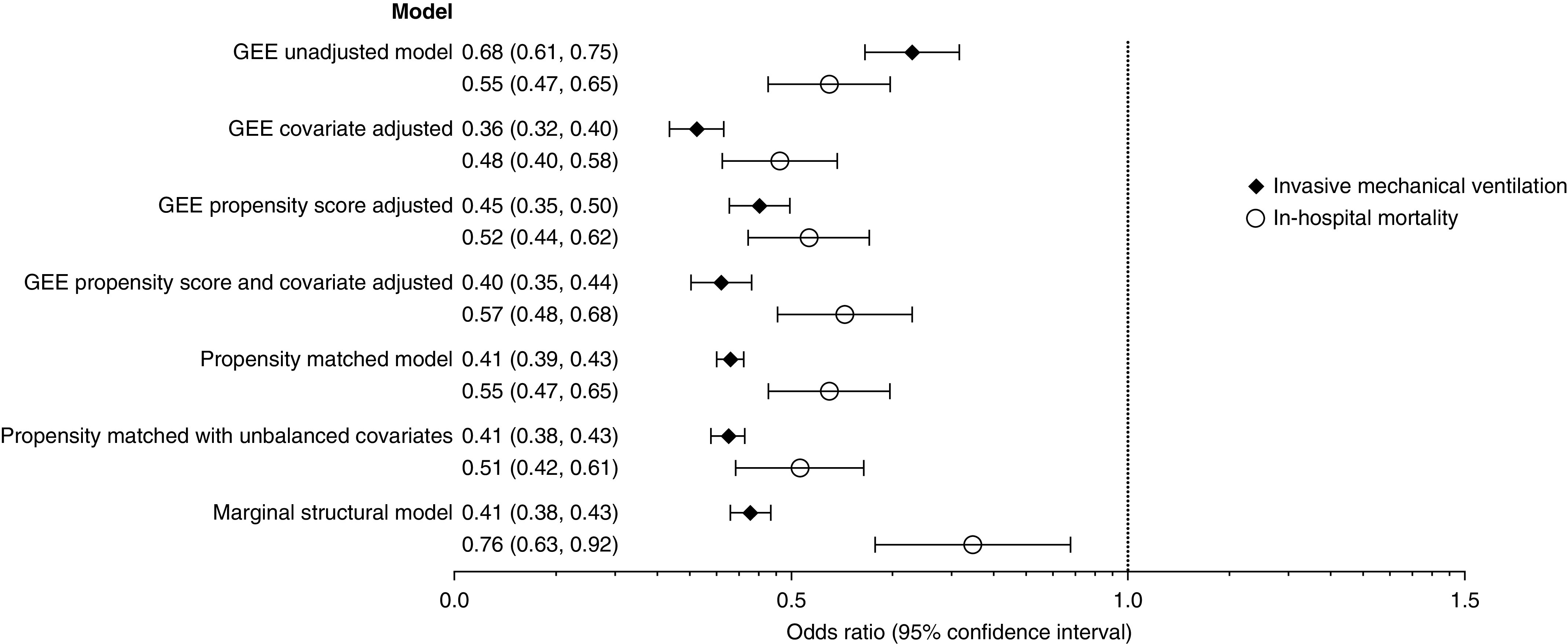
Rationale: Noninvasive ventilation decreases the need for invasive mechanical ventilation and mortality among patients with chronic obstructive pulmonary disease but has not been well studied in asthma.Objectives: To assess the association between noninvasive ventilation and subsequent need for invasive mechanical ventilation and in-hospital mortality among patients admitted with asthma exacerbation to the ICU.Methods: We performed a retrospective cohort study using administrative data collected during 2010-2017 from 682 hospitals in the United States. Outcomes included receipt of invasive mechanical ventilation and in-hospital mortality. Generalized estimating equations, propensity-matched models, and marginal structural models were used to assess the association between noninvasive ventilation and outcomes.Measurements and Main Results: The study population included 53,654 participants with asthma exacerbation. During the study period, 13,540 patients received noninvasive ventilation (25.2%; 95% confidence interval [CI], 24.9-25.6%), 14,498 underwent invasive mechanical ventilation (27.0%; 95% CI, 26.7-27.4%), and 1,291 died (2.4%; 95% CI, 2.3-2.5%). Among those receiving noninvasive ventilation, 3,013 patients (22.3%; 95% CI, 21.6-23.0%) required invasive mechanical ventilation after first receiving noninvasive ventilation, 136 of whom died (4.5%; 95% CI, 3.8-5.3%). Across all models, the use of noninvasive ventilation was associated with a lower odds of receiving invasive mechanical ventilation (adjusted generalized estimating equation odds ratio, 0.36; 95% CI, 0.32-0.40) and in-hospital mortality (odds ratio, 0.48; 95% CI 0.40-0.58). Those who received noninvasive ventilation before invasive mechanical ventilation were more likely to have comorbid pneumonia and severe sepsis.Conclusions: Noninvasive ventilation use during asthma exacerbation was associated with improved outcomes but should be used cautiously with acute comorbid conditions.
Keywords: continuous positive airway pressure; critical care outcomes; mechanical ventilators; respiratory insufficiency; retrospective studies.
Figures
Comment in
-
Noninvasive Ventilation for Acute Asthma: The Neglected Sibling.Am J Respir Crit Care Med. 2020 Dec 1;202(11):1491-1493. doi: 10.1164/rccm.202007-2876ED. Am J Respir Crit Care Med. 2020. PMID: 32755489 Free PMC article. No abstract available.
References
-
- Akinbami LJ, Moorman JE, Bailey C, Zahran HS, King M, Johnson CA, et al. Trends in asthma prevalence, health care use, and mortality in the United States, 2001-2010 NCHS Data Brief 2012. 94):1–8. - PubMed
-
- Epidemiology and Statistics Unit, Research and Health Education Division, American Lung Association. Trends in asthma morbidity and mortality. September 2012 [accessed 2018 Feb 22]. Available from: https://www.lung.org/research/trends-in-lung-disease/asthma-trends-brief....
-
- Rodrigo GJ, Rodrigo C, Hall JB. Acute asthma in adults: a review. Chest. 2004;125:1081–1102. - PubMed
