

Is the COVID-19 Pandemic a Good Time to Include Aspergillus Molecular Detection to Categorize Aspergillosis in ICU Patients? A Monocentric Experience
- PMID: 32664423
- PMCID: PMC7558333
- DOI: 10.3390/jof6030105
Is the COVID-19 Pandemic a Good Time to Include Aspergillus Molecular Detection to Categorize Aspergillosis in ICU Patients? A Monocentric Experience
Abstract
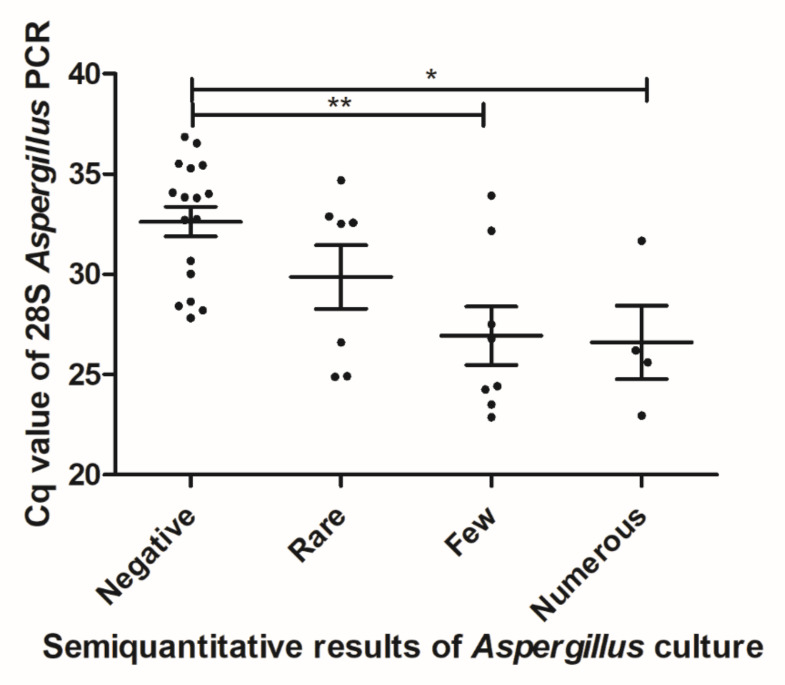
(1) Background: The diagnosis of invasive aspergillosis (IA) in an intensive care unit (ICU)remains a challenge and the COVID-19 epidemic makes it even harder. Here, we evaluatedAspergillus PCR input to help classifying IA in SARS-CoV-2-infected patients. (2) Methods: 45COVID-19 patients were prospectively monitored twice weekly for Aspergillus markers and anti-Aspergillus serology. We evaluated the concordance between (Ι) Aspergillus PCR and culture inrespiratory samples, and (ΙΙ) blood PCR and serum galactomannan. Patients were classified asputative/proven/colonized using AspICU algorithm and two other methods. (3) Results: Theconcordance of techniques applied on respiratory and blood samples was moderate (kappa = 0.58and kappa = 0.63, respectively), with a higher sensitivity of PCR. According to AspICU, 9/45 patientswere classified as putative IA. When incorporating PCR results, 15 were putative IA because theymet all criteria, probably with a lack of specificity in the context of COVID-19. Using a modifiedAspICU algorithm, eight patients were classified as colonized and seven as putative IA. (4)Conclusion: An appreciation of the fungal burden using PCR and Aspergillus serology was addedto propose a modified AspICU algorithm. This proof of concept seemed relevant, as it was inagreement with the outcome of patients, but will need validation in larger cohorts.
Keywords: Aspergillus; COVID-19; ICU; PCR; Sars-CoV-2; classification; galactomannan; invasive aspergillosis; probable; putative.
Conflict of interest statement
J.-P.G. received funds for communications and congress attendance from Pfizer and Gilead. The other authors declare they have no conflict of interest.
Figures
References
-
- White P.L., Wingard J.R., Bretagne S., Löffler J., Patterson T.F., Slavin M.A., Barnes R.A., Pappas P.G., Donnelly J.P. Aspergillus Polymerase Chain Reaction: Systematic Review of Evidence for Clinical Use in Comparison With Antigen Testing. J. Clin. Microbiol. 2015;61:1293–1303. doi: 10.1093/cid/civ507. - DOI - PMC - PubMed
-
- Donnelly J.P., Chen S.C., Kauffman C.A., Steinbach W.J., Baddley J.W., Verweij P.E., Clancy C.J., Wingard J.R., Lockhart S.R., Groll A.H., et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2019:ciz1008. doi: 10.1093/cid/ciz1008. - DOI - PMC - PubMed
-
- Blot S., Taccone F., Van den Abeele A., Meersseman W., Brusselaers W., Dimopoulos G., Paiva J., Misset B., Rello J., Vandewoude K., et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2012;186:56–64. doi: 10.1164/rccm.201111-1978OC. - DOI - PubMed
-
- Bulpa P., Bihin B., Dimopoulos G., Taccone F.S., Van den Abeele A.-M., Misset B., Meersseman W., Spapen H., Cardoso T., Charles P.-E., et al. Which algorithm diagnoses invasive pulmonary aspergillosis best in ICU patients with COPD? Eur. Respir. J. 2017;50:1700532. doi: 10.1183/13993003.00532-2017. - DOI - PubMed
-
- Bassetti M., Giacobbe D.R., Grecchi C., Rebuffi C., Zuccaro V., Scudeller L., FUNDICU Investigators Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: A systematic review with qualitative evidence synthesis. J. Infect. 2020 doi: 10.1016/j.jinf.2020.03.065. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
