

New insights into genetic susceptibility of COVID-19: an ACE2 and TMPRSS2 polymorphism analysis
- PMID: 32664879
- PMCID: PMC7360473
- DOI: 10.1186/s12916-020-01673-z
New insights into genetic susceptibility of COVID-19: an ACE2 and TMPRSS2 polymorphism analysis
Abstract
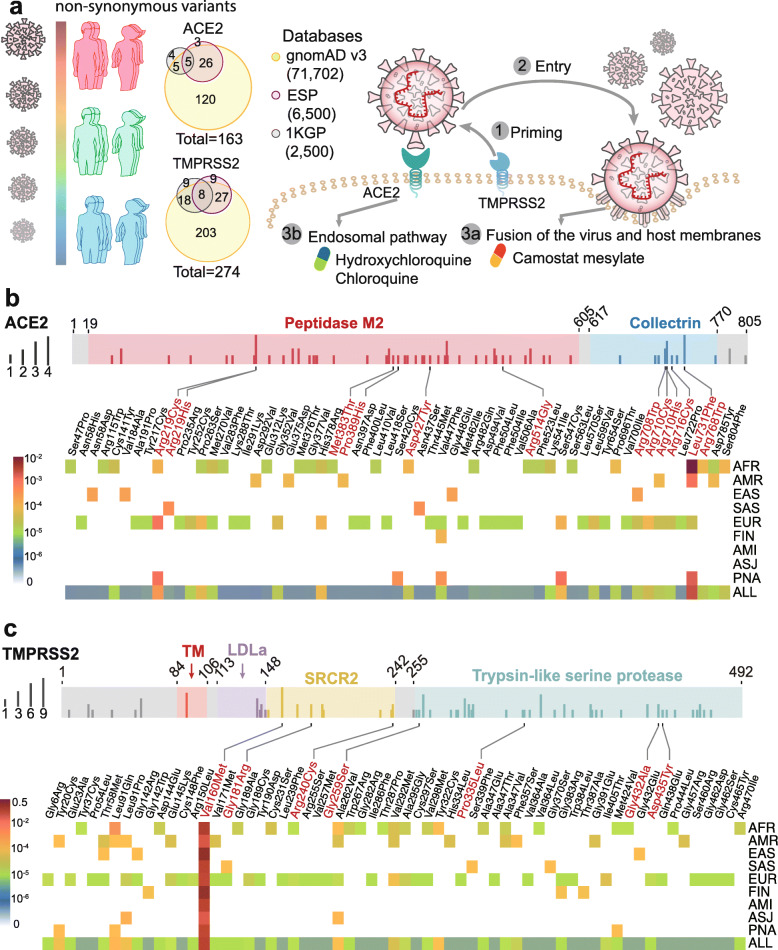
Background: Coronavirus Disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has now been confirmed worldwide. Yet, COVID-19 is strangely and tragically selective. Morbidity and mortality due to COVID19 rise dramatically with age and co-existing health conditions, including cancer and cardiovascular diseases. Human genetic factors may contribute to the extremely high transmissibility of SARS-CoV-2 and to the relentlessly progressive disease observed in a small but significant proportion of infected individuals, but these factors are largely unknown.
Main body: In this study, we investigated genetic susceptibility to COVID-19 by examining DNA polymorphisms in ACE2 and TMPRSS2 (two key host factors of SARS-CoV-2) from ~ 81,000 human genomes. We found unique genetic susceptibility across different populations in ACE2 and TMPRSS2. Specifically, ACE2 polymorphisms were found to be associated with cardiovascular and pulmonary conditions by altering the angiotensinogen-ACE2 interactions, such as p.Arg514Gly in the African/African-American population. Unique but prevalent polymorphisms (including p.Val160Met (rs12329760), an expression quantitative trait locus (eQTL)) in TMPRSS2, offer potential explanations for differential genetic susceptibility to COVID-19 as well as for risk factors, including those with cancer and the high-risk group of male patients. We further discussed that polymorphisms in ACE2 or TMPRSS2 could guide effective treatments (i.e., hydroxychloroquine and camostat) for COVID-19.
Conclusion: This study suggested that ACE2 or TMPRSS2 DNA polymorphisms were likely associated with genetic susceptibility of COVID-19, which calls for a human genetics initiative for fighting the COVID-19 pandemic.
Keywords: Angiotensin-converting enzyme 2 (ACE2); COVID-19; Coronavirus; Genetic susceptibility; SARS-CoV-2; TMPRSS2.
Conflict of interest statement
The content of this publication does not necessarily reflect the views of the Cleveland Clinic. The authors declare no competing interests.
Figures

References
-
- Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, Tong S. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;8(6):2118–2120. - PubMed
-
- Hoffmann M, Kleine-Weber H, Schroeder S, Kruger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–280. doi: 10.1016/j.cell.2020.02.052. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
