

Multicenter evaluation of a syndromic rapid multiplex PCR test for early adaptation of antimicrobial therapy in adult patients with pneumonia
- PMID: 32665030
- PMCID: PMC7359443
- DOI: 10.1186/s13054-020-03114-y
Multicenter evaluation of a syndromic rapid multiplex PCR test for early adaptation of antimicrobial therapy in adult patients with pneumonia
Abstract
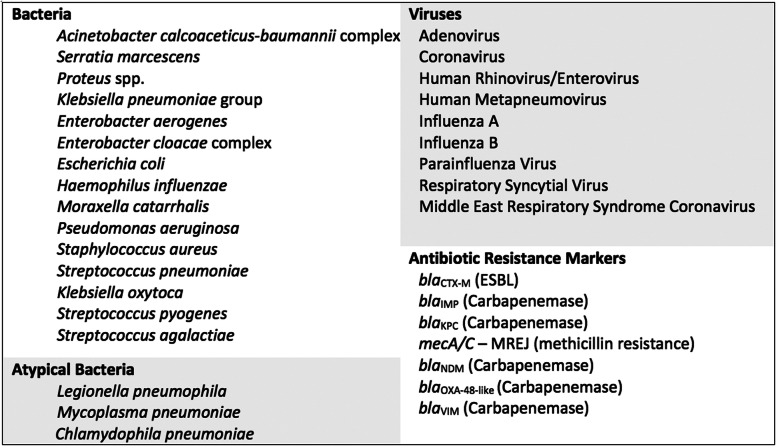
Background: Improving timeliness of pathogen identification is crucial to allow early adaptation of antibiotic therapy and improve prognosis in patients with pneumonia. We evaluated the relevance of a new syndromic rapid multiplex PCR test (rm-PCR) on respiratory samples to guide empirical antimicrobial therapy in adult patients with community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP), and ventilator-acquired pneumonia (VAP).
Methods: This retrospective multicenter study was conducted in four French university hospitals. Respiratory samples were obtained from patients with clinical and radiological signs of pneumonia and simultaneously tested using conventional microbiological methods and the rm-PCR. A committee composed of an intensivist, a microbiologist, and an infectious diseases specialist retrospectively assessed all medical files and agreed on the most appropriate antimicrobial therapy for each pneumonia episode, according to the results of rm-PCR and blinded to the culture results. The rm-PCR-guided antimicrobial regimen was compared to the empirical treatment routinely administered to the patient in standard care.
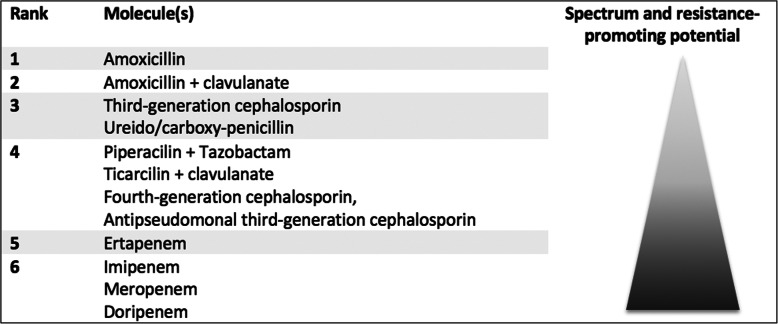
Results: We included 159 pneumonia episodes. Most patients were hospitalized in intensive care units (n = 129, 81%), and episodes were HAP (n = 68, 43%), CAP (n = 54, 34%), and VAP (n = 37, 23%). Conventional culture isolated ≥ 1 microorganism(s) at significant level in 95 (60%) patients. The syndromic rm-PCR detected at least one bacteria in 132 (83%) episodes. Based on the results of the rm-PCR, the multidisciplinary committee proposed a modification of the empirical therapy in 123 (77%) pneumonia episodes. The modification was a de-escalation in 63 (40%), an escalation in 35 (22%), and undetermined in 25 (16%) patients. In microbiologically documented episodes (n = 95), the rm-PCR increased appropriateness of the empirical therapy to 83 (87%), as compared to 73 (77%) in routine care.
Conclusions: Use of a syndromic rm-PCR test has the potential to reduce unnecessary antimicrobial exposure and increase the appropriateness of empirical antibiotic therapy in adult patients with pneumonia.
Keywords: Antimicrobial stewardship; Antimicrobials; Biofire® FilmArray®; Multiplex PCR; Pneumonia; Syndromic tests.
Conflict of interest statement
bioMerieux SA provided IUO tests for the study. bioMerieux SA did not interfere with data collection and analysis, nor with manuscript preparation. Dr. Julien Textoris participated in the elaboration of the protocol.
SK declares grants from bioMérieux and lecture fees and conference invitations from bioMérieux, MSD, and Accelerate Diagnostics.
CM received lecture fees from bioMerieux SA.
ATD and NG report no conflicts of interest.
VC reports personal fees from Accelerate Diagnostics, Astellas, bioMérieux, Correvio, Curetis, Eumédica, Menarini, Mylan, Pfizer, and Sanofi.
LA received lecture fees from Pfizer, MSD, Biocodex, and Biomerieux.
All authors have submitted the ICMJE form for disclosure of potential conflicts of interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61–111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
-
- Torres A, Niederman MS, Chastre J, Ewig S, Fernandez-Vandellos P, Hanberger H, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017;50:1700582. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
