

The effect of temporary closure and enhanced terminal disinfection using aerosolized hydrogen peroxide of an open-bay intensive care unit on the acquisition of extensively drug-resistant Acinetobacter baumannii
- PMID: 32665037
- PMCID: PMC7362486
- DOI: 10.1186/s13756-020-00772-z
The effect of temporary closure and enhanced terminal disinfection using aerosolized hydrogen peroxide of an open-bay intensive care unit on the acquisition of extensively drug-resistant Acinetobacter baumannii
Abstract
Background: At Makassed Hospital's open-bay intensive care unit (ICU), enhanced terminal disinfection (ETD) using hydrogen peroxide (H2O2) was performed without a predefined schedule in extensively-drug-resistant Acinetobacter baumannii (XDR-AB) outbreaks. In this study, we aimed to check for the value of the temporary closure of the ICU and the use of ETD with aerosolized H2O2 and Ag+ on minimizing the rate of XDR-AB acquisition in patients admitted to the ICU of our facility, which might consequently help us determine the optimal schedule for such procedure in this unit.
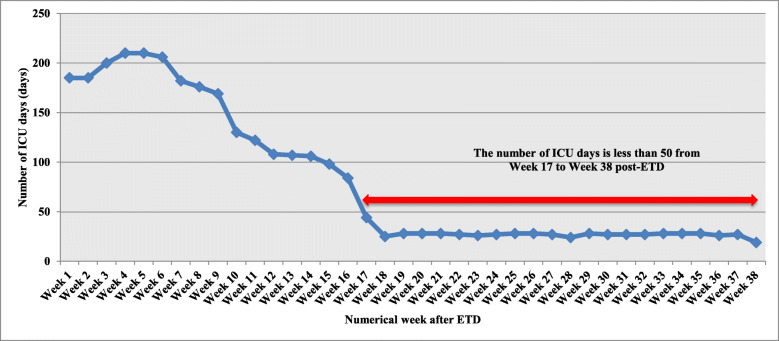
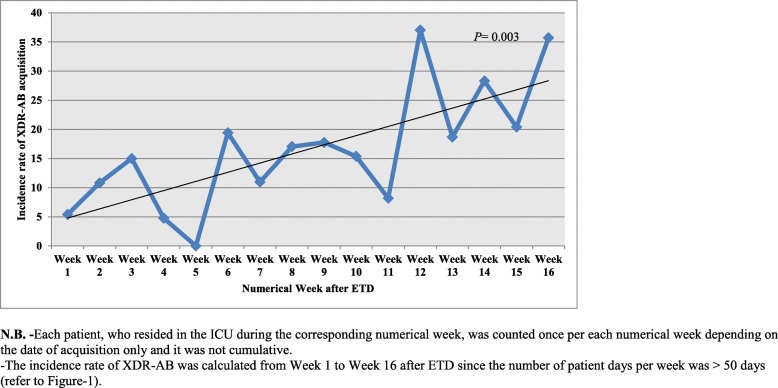
Methods: This is a retrospective medical file review of patients admitted to the ICU between January 2016 and May 2018. We divided this period into numerical weeks (NW) after each closure and ETD episode. Risk factors of acquisition (RFA) were determined by comparing the characteristics of patients who acquired XDR-AB to those who didn't. The proportion of patients residing in each NW was included in the RFA analysis.
Results: Out of 335 patients, 13% acquired XDR-AB. The overall incidence of XDR-AB acquisition was 14.6 cases/1000 patient days. RFA were XDR-AB contact pressure ≥ 3 days [Odds Ratio (OR) = 9.86, 95% Confidence Interval (CI) (3.65-26.64), P < 0.0001)], mechanical ventilation [OR = 4.99, 95%CI (1.76-14.15), P = 0.002)], and having a wound [OR = 3.72, 95%CI (0.99-13.96), P = 0.05)]. Patients who stayed during NW 7,11 and 14 were at risk of acquisition where the odds significantly increased by 6.5, 9.7 and 14.4 folds respectively (P = 0.03,0.01, and 0.01, respectively). We considered NW 7 as the most suitable time for temporary closure of the ICU and ETD with aerosolized H2O2.
Conclusion: Contact pressure, mechanical ventilation, and presence of a wound were RFA of XDR-AB. Temporary closure of the ICU with ETD using aerosolized H2O2 decreased the rate of XDR-AB acquisition, yet this effect fades away with time. The ETD was shown to be most efficiently done when repeated every 7 calendar weeks in our open-bay ICU as part of a prevention bundle.
Keywords: Contact pressure; Enhanced terminal disinfection; Extensively drug-resistant Acinetobacter baumannii; Hydrogen peroxide; Intensive care unit; Lebanon; Open-bay.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO . Global antimicrobial resistance surveillance system (GLASS) report. 2018.
-
- Moghnieh R, Siblani L, Ghadban D, et al. Extensively drug-resistant Acinetobacter baumannii in a Lebanese intensive care unit: risk factors for acquisition and determination of a colonization score. J Hosp Infect. 2016;92(1):47–53. - PubMed
-
- Al Atrouni A, Hamze M, Jisr T, et al. Wide spread of OXA-23-producing carbapenem-resistant Acinetobacter baumannii belonging to clonal complex II in different hospitals in Lebanon. Int J Infect Dis. 2016;52:29–36. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
