

Renal hyperfiltration is independently associated with increased all-cause mortality in individuals with type 2 diabetes: a prospective cohort study
- PMID: 32665314
- PMCID: PMC7365485
- DOI: 10.1136/bmjdrc-2020-001481
Renal hyperfiltration is independently associated with increased all-cause mortality in individuals with type 2 diabetes: a prospective cohort study
Abstract
Introduction: In addition to favoring renal disease progression, renal 'hyperfiltration' has been associated with an increased risk of death, though it is unclear whether and how excess mortality is related to increased renal function. We investigated whether renal hyperfiltration is an independent predictor of death in patients with type 2 diabetes from the Renal Insufficiency And Cardiovascular Events Italian multicenter study.
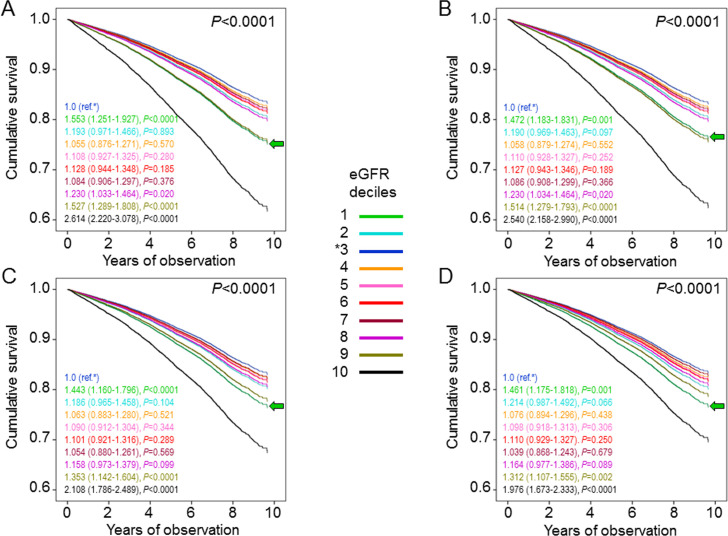
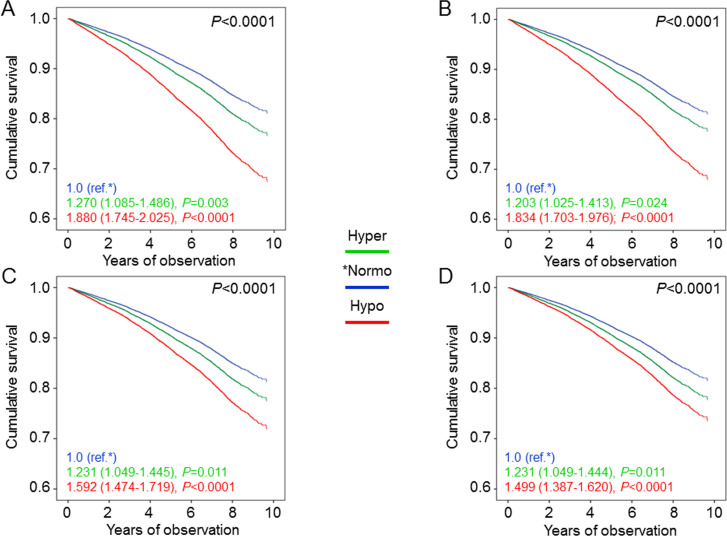
Research design and methods: This observational, prospective cohort study enrolled 15 773 patients with type 2 diabetes consecutively attending 19 Italian diabetes clinics in 2006-2008. Serum creatinine, albuminuria, cardiovascular risk factors, and complications/comorbidities were assessed at baseline. Vital status on 31 October 2015 was retrieved for 15 656 patients (99.26%). Patients were stratified (A) by absolute estimated glomerular filtration rate (eGFR) values in eGFR deciles or Kidney Disease: Improving Global Outcomes (KDIGO) categories and (B) based on age-corrected thresholds or age and gender-specific 95th and 5th percentiles in hyperfiltration, hypofiltration, and normofiltration groups.
Results: The highest eGFR decile/category and the hyperfiltration group included (partly) different individuals with similar clinical features. Age and gender-adjusted death rates were significantly higher in deciles 1, 9, and 10 (≥103.9, 50.9-62.7, and <50.9 mL/min/1.73 m2, respectively) versus the reference decile 3 (92.9-97.5 mL/min/1.73 m2). Mortality risk, adjusted for multiple confounders, was also increased in deciles 1 (HR 1.461 (95% CI 1.175 to 1.818), p=0.001), 9 (1.312 (95% CI 1.107 to 1.555), p=0.002), and 10 (1.976 (95% CI 1.673 to 2.333), p<0.0001) versus decile 3. Similar results were obtained by stratifying patients by KDIGO categories. Death rates and adjusted mortality risks were significantly higher in hyperfiltering and particularly hypofiltering versus normofiltering individuals.
Conclusions: In type 2 diabetes, both high-normal eGFR and hyperfiltration are associated with an increased risk of death from any cause, independent of confounders that may directly impact on mortality and/or affect GFR estimation. Further studies are required to clarify the nature of this relationship.
Trial registration number: NCT00715481.
Keywords: diabetes mellitus, type 2; kidney diseases; mortality.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GPe: lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Sigma-Tau, and Takeda, and travel grants from AstraZeneca, Novo Nordisk, and Takeda. EO: consultant fees from Eli Lilly and Novo Nordisk. AS: consultant fees from AstraZeneca, Boehringer Ingelheim, and Sanofi-Aventis, and lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Mundipharma. EB: consultant fees from Abbott, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Bruno Farmaceutici, Eli Lilly, Janssen, Johnson & Johnson, Merck Sharp & Dohme, Mundipharma, Novartis, Novo Nordisk, Roche, Sanofi-Aventis, Servier, and Takeda, and research grants from AstraZeneca, Genzyme, Menarini Diagnostics, Novo Nordisk, Roche, and Takeda. CF: lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk and travel grants from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Sanofi-Aventis, and Takeda. RT: consultant fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, and Sanofi-Aventis, and lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk. MV: lecture fees from LifeScan and Novo Nordisk. FC: lecture fees from AstraZeneca, Sanofi-Aventis, and Takeda. GG: lecture fees from Boehringer Ingelheim and Mundipharma. LL: consultant fees from Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Medtronic, Movi, Novo Nordisk, Roche, Sanofi-Aventis, and Takeda, and lecture fees from Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Medtronic, Menarini, Merck Sharp & Dohme, Movi, Mundipharma, Novo Nordisk, Roche, Sanofi-Aventis, and Takeda. AN: consultant fees from AstraZeneca, Pikdare, Roche, lecture fees from AstraZeneca, Boehringer Ingelheim, Medtronic, and Novo Nordisk, and research grants from Aboca, AstraZeneca, Eli Lilly, Novo Nordisk, Sanofi-Aventis, and Theras. GPu: consultant fees from AstraZeneca, Boehringer Ingelheim, and Eli Lilly, lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Mundipharma, Novartis, Novo Nordisk, Sigma-Tau, Takeda, and travel grants from AstraZeneca, Laboratori Guidotti, Sanofi-Aventis, and Takeda.
Figures
Similar articles
-
Non-albuminuric renal impairment is a strong predictor of mortality in individuals with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian multicentre study.Diabetologia. 2018 Nov;61(11):2277-2289. doi: 10.1007/s00125-018-4691-2. Epub 2018 Jul 21. Diabetologia. 2018. PMID: 30032426
-
Insulin resistance, diabetic kidney disease, and all-cause mortality in individuals with type 2 diabetes: a prospective cohort study.BMC Med. 2021 Mar 15;19(1):66. doi: 10.1186/s12916-021-01936-3. BMC Med. 2021. PMID: 33715620 Free PMC article.
-
Defining the contribution of chronic kidney disease to all-cause mortality in patients with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian Multicenter Study.Acta Diabetol. 2018 Jun;55(6):603-612. doi: 10.1007/s00592-018-1133-z. Epub 2018 Mar 24. Acta Diabetol. 2018. PMID: 29574497
-
The renoprotective effects of sodium-glucose cotransporter 2 inhibitors versus placebo in patients with type 2 diabetes with or without prevalent kidney disease: A systematic review and meta-analysis.Diabetes Obes Metab. 2019 Apr;21(4):1018-1026. doi: 10.1111/dom.13620. Epub 2019 Jan 16. Diabetes Obes Metab. 2019. PMID: 30565382
-
Renal hyperfiltration defined by high estimated glomerular filtration rate: A risk factor for cardiovascular disease and mortality.Diabetes Obes Metab. 2019 Nov;21(11):2368-2383. doi: 10.1111/dom.13831. Epub 2019 Jul 29. Diabetes Obes Metab. 2019. PMID: 31297976
Cited by
-
A Cross-Sectional Study of Glomerular Hyperfiltration in Polycystic Ovary Syndrome.Int J Mol Sci. 2024 Apr 30;25(9):4899. doi: 10.3390/ijms25094899. Int J Mol Sci. 2024. PMID: 38732117 Free PMC article.
-
Sex-specific association of body mass index and fatty liver index with prevalence of renal hyperfiltration: a cross sectional study using Japanese health check-up data.BMC Nephrol. 2023 Apr 3;24(1):85. doi: 10.1186/s12882-023-03137-x. BMC Nephrol. 2023. PMID: 37013497 Free PMC article.
-
Glomerular Biomechanical Stress and Lipid Mediators during Cellular Changes Leading to Chronic Kidney Disease.Biomedicines. 2022 Feb 9;10(2):407. doi: 10.3390/biomedicines10020407. Biomedicines. 2022. PMID: 35203616 Free PMC article. Review.
-
Finerenone: Questions and Answers-The Four Fundamental Arguments on the New-Born Promising Non-Steroidal Mineralocorticoid Receptor Antagonist.J Clin Med. 2023 Jun 12;12(12):3992. doi: 10.3390/jcm12123992. J Clin Med. 2023. PMID: 37373685 Free PMC article. Review.
-
Approaches to predict future type 2 diabetes mellitus and chronic kidney disease: A scoping review.PLoS One. 2025 Jun 11;20(6):e0325182. doi: 10.1371/journal.pone.0325182. eCollection 2025. PLoS One. 2025. PMID: 40498698 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous