

Long-term outcomes in patients with polyarticular juvenile idiopathic arthritis receiving adalimumab with or without methotrexate
- PMID: 32665432
- PMCID: PMC7425194
- DOI: 10.1136/rmdopen-2020-001208
Long-term outcomes in patients with polyarticular juvenile idiopathic arthritis receiving adalimumab with or without methotrexate
Abstract
Objectives: Long-term safety and efficacy of adalimumab among patients with juvenile idiopathic arthritis (JIA) was evaluated through 6 years of treatment.
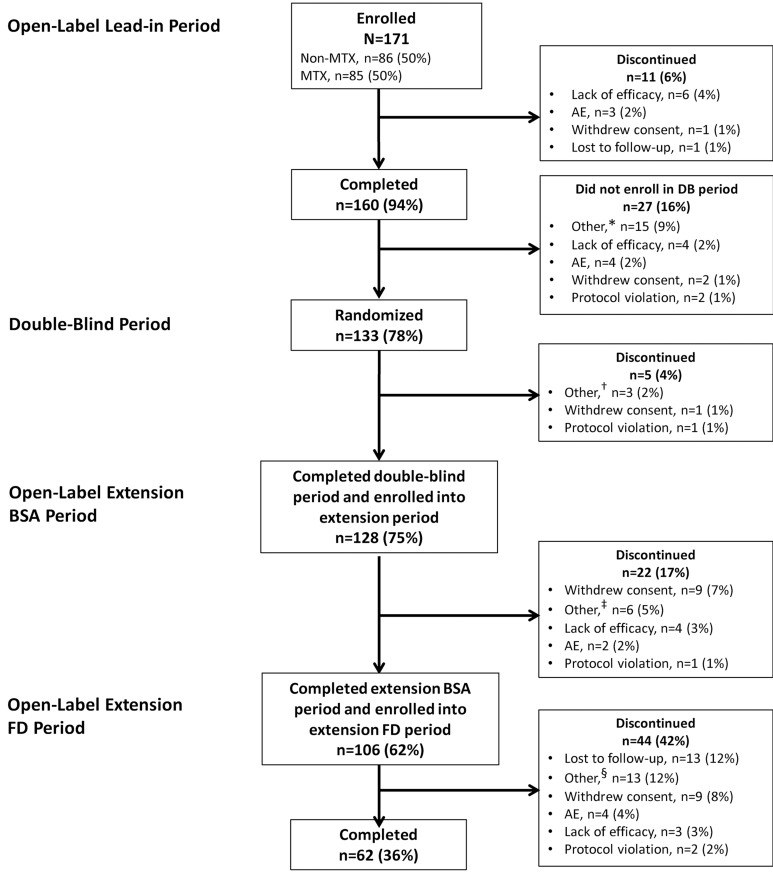
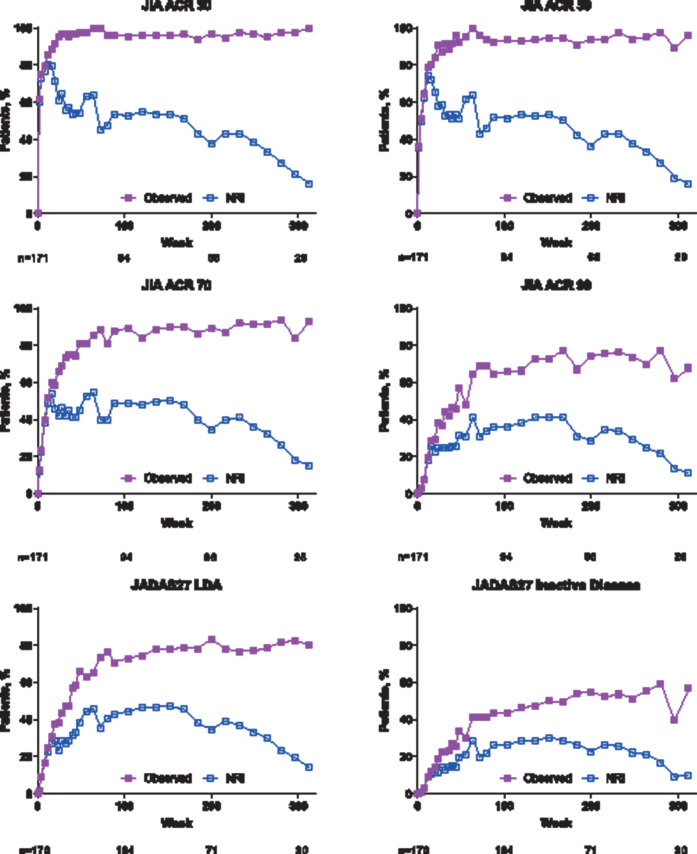
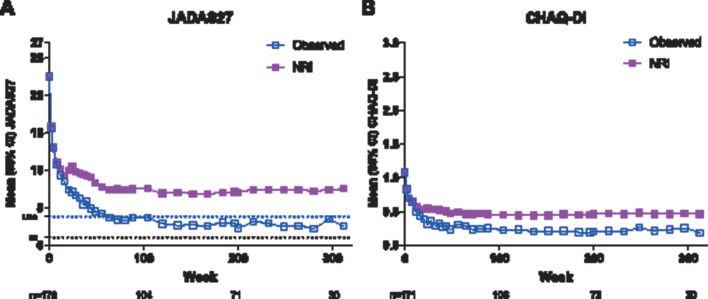
Methods: Children aged 4-17 years with polyarticular JIA were enrolled in a phase III, randomised-withdrawal, double-blind, placebo-controlled trial consisting of a 16-week open-label lead-in period, 32-week randomised double-blind period and 360-week long-term extension. Patients were stratified by baseline methotrexate use. Adverse events (AEs) were monitored, and efficacy assessments included JIA American College of Rheumatology (JIA ACR) 30%, 50%, 70% or 90% responses and the proportions of patients achieving 27-joint Juvenile Arthritis Disease Activity Score (JADAS27) low disease activity (LDA, ≤3.8) and inactive disease (ID, ≤1).
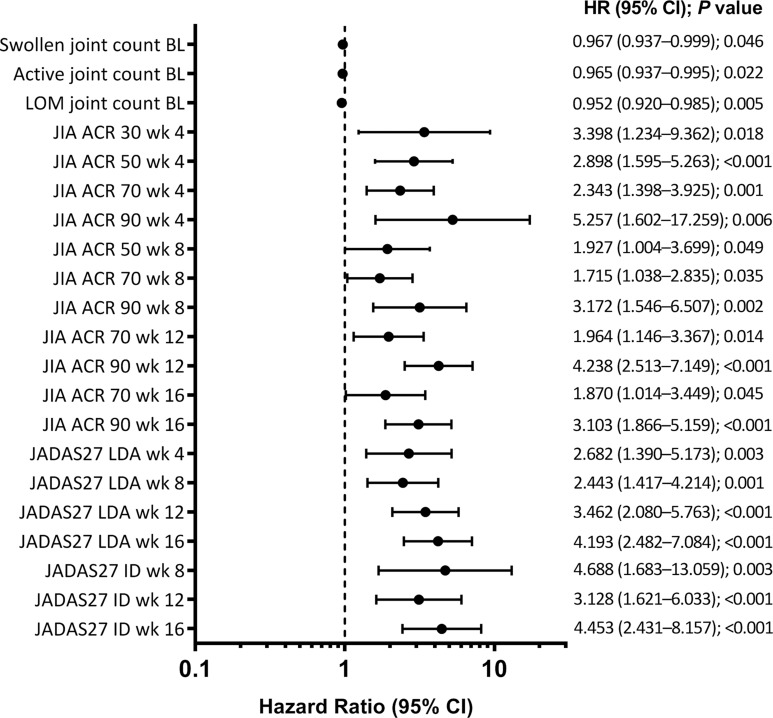
Results: Of 171 patients enrolled, 62 (36%) completed the long-term extension. Twelve serious infections in 11 patients were reported through 592.8 patient-years of exposure. No cases of congestive heart failure-related AEs, demyelinating disease, lupus-like syndrome, malignancies, tuberculosis or deaths were reported. JIA ACR 30/50/70/90 responses and JADAS27 LDA were achieved in 66% to 96% of patients at week 104, and 63 (37%) patients achieved clinical remission (JADAS27 ID sustained for ≥6 continuous months) during the study. Attainment of JIA ACR 50 or higher and JADAS27 LDA or ID in the initial weeks were the best predictors of clinical remission. Mean JADAS27 decreased from baseline, 22.5 (n=170), to 2.5 (n=30) at week 312 (observed analysis).
Conclusions: Through 6 years of exposure, adalimumab was well tolerated with significant clinical response (up to clinical remission) and a relatively low retention rate.
Keywords: Adult Onset Still’s Disease; Anti-TNF; Arthritis; Autoimmune Diseases; Dermatomyositis; Familial Mediterranean Fever; Juvenile Idiopathic Arthritis; Lupus Erythematosus; Methotrexate; Systemic.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: DJL has served on speakers’ bureaus for Genentech and Bristol-Myers Squibb and on data and safety monitoring boards for Forest Research and the National Institutes of Health-NIAMS. Cincinnati Children’s Hospital Medical Center has received consulting fees from AbbVie, AstraZeneca, Centocor, Bristol-Myers Squibb, Pfizer, Regeneron, Hoffman La-Roche, Novartis, UBC, Xoma and Genentech for the work of DJL.HIB has received speaker honoraria and consulting fees from AbbVie, AstraZeneca, Centocor, Bristol-Myers Squibb, Boehringer Ingelheim, Pfizer, Regeneron, Hoffman La-Roche, Novartis, Takeda, UCB, Genentech, Lilly, Janssen, EMD Serono and R-Pharm; and has served on speakers bureaus for Genentech and Novartis.AOR has received consulting fees and speaker fees from AbbVie and Novartis.LJ has served as a consultant for OncoImmune and Novartis; has received unrestricted education grants from AbbVie; has received clinical trial support from AbbVie, Bristol-Myers Squibb and UCB Biosciences; and has served on a data and safety monitoring board for Bristol-Myers Squibb.KJ has nothing to disclose.DN has nothing to disclose.RM has received honoraria from AbbVie as a co-investigator during this clinical trial.CS has nothing to disclose.JFB has nothing to disclose.DE has received research grants, consulting fees and/or speakers fees from AbbVie.CG has nothing to disclose.GH has nothing to declare.IK-P has received consulting fees from AbbVie, Pfizer, Roche, CHUGAI, Novartis, SOBI and Novimmune.OYJ has nothing to disclose.VV has received speaker fees from AbbVie and Pfizer.EC has received speaker fees from AbbVie.CW has received research grants to her institution from Roche, Pfizer and GSK.IL and YS are full-time employees of AbbVie and may hold stock or stock options.AM is a professor of pediatrics at the University of Genoa, Italy, and has consultancy agreements with Janssen, Novartis and Pfizer. Prior to January 2019, AM was a scientific director of the Giannina Gaslini Hospital and performed consultancy activities on behalf of the Gaslini Institute for the following companies: AbbVie, Biogen, Boehringer, Bristol-Myers Squibb, EMD Serono, Janssen, Novartis, Pfizer, and R-Pharm.NR is a full-time employee of the Gaslini Hospital, which has received contributions to support the research activities of the network of PRINTO from AbbVie, AstraZeneca, Bristol-Myers Squibb, Janssen Biologics B.V., Eli Lilly and Co., ‘Francesco Angelini’, GlaxoSmithKline, Italfarmaco, Novartis, Pfizer, Roche, Sanofi Aventis, Schwarz Biosciences GmbH, Xoma and Wyeth Pharmaceuticals. NR has served on speakers bureaus for Astellas, AstraZeneca, Bristol-Myers Squibb, Italfarmaco, Janssen Biologics B.V., MedImmune, Roche and Wyeth/Pfizer.
Figures
References
-
- Martini A, Ravelli A, Avcin T, et al. Toward new classification criteria for juvenile idiopathic arthritis: first steps, Pediatric Rheumatology International Trials Organization international consensus. J Rheumatol 2018. - PubMed
-
- Ringold S, Angeles-Han ST, Beukelman T, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the treatment of juvenile idiopathic arthritis: therapeutic approaches for non-systemic polyarthritis, sacroiliitis, and enthesitis. Arthritis Care Res (Hoboken) 2019;71:717–34. - PMC - PubMed
-
- Hashkes PJ, Laxer RM. Medical treatment of juvenile idiopathic arthritis. JAMA 2005;294:1671–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical