

Transplacental transmission of SARS-CoV-2 infection
- PMID: 32665677
- PMCID: PMC7360599
- DOI: 10.1038/s41467-020-17436-6
Transplacental transmission of SARS-CoV-2 infection
Abstract
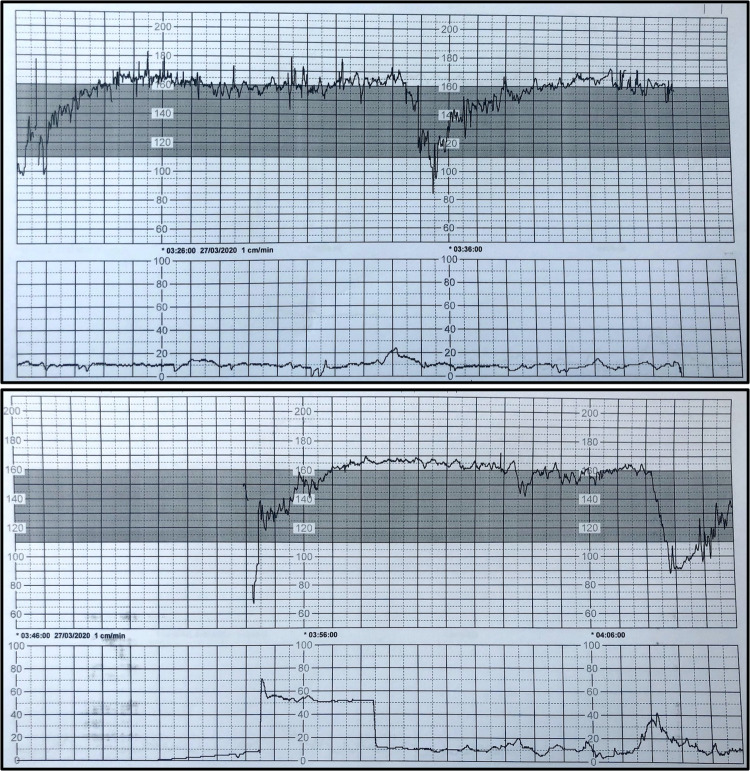
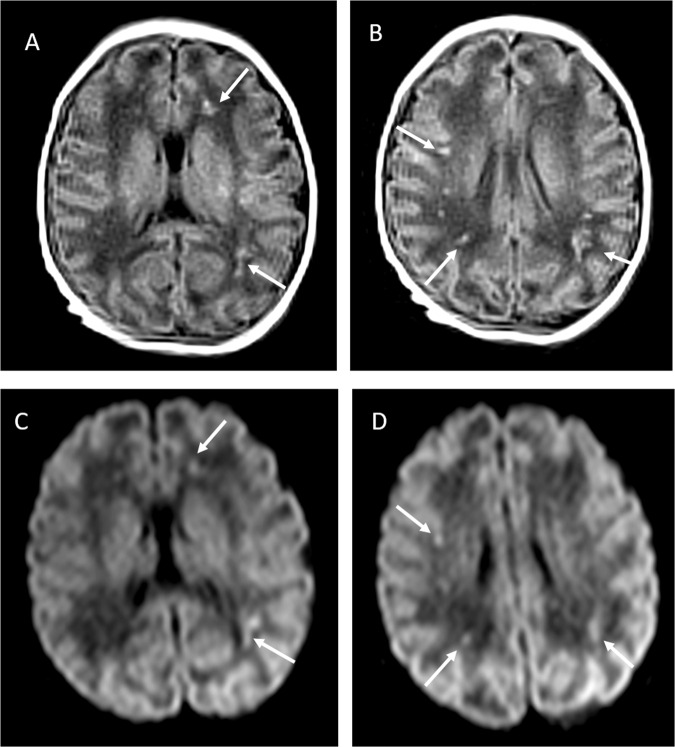
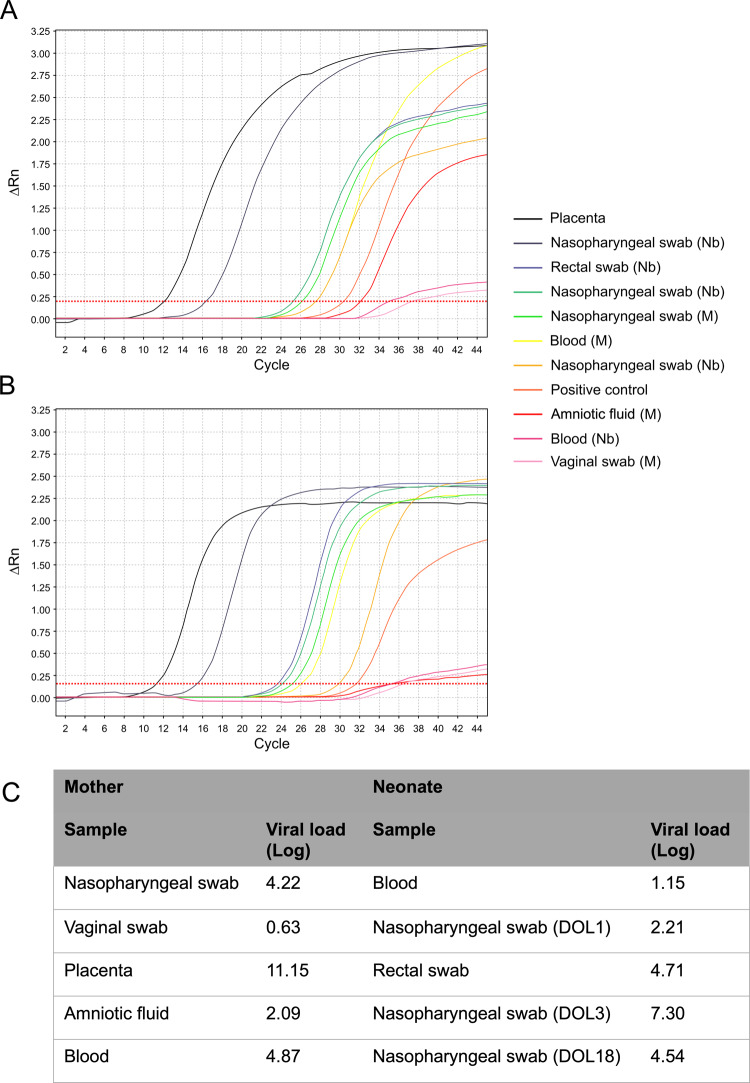
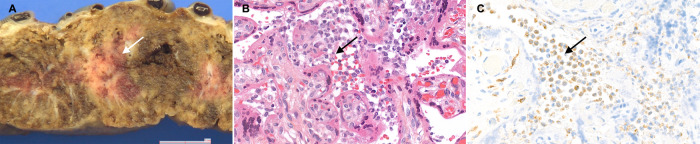
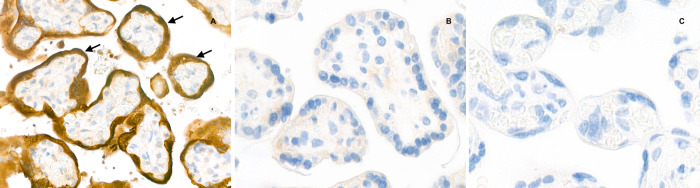
SARS-CoV-2 outbreak is the first pandemic of the century. SARS-CoV-2 infection is transmitted through droplets; other transmission routes are hypothesized but not confirmed. So far, it is unclear whether and how SARS-CoV-2 can be transmitted from the mother to the fetus. We demonstrate the transplacental transmission of SARS-CoV-2 in a neonate born to a mother infected in the last trimester and presenting with neurological compromise. The transmission is confirmed by comprehensive virological and pathological investigations. In detail, SARS-CoV-2 causes: (1) maternal viremia, (2) placental infection demonstrated by immunohistochemistry and very high viral load; placental inflammation, as shown by histological examination and immunohistochemistry, and (3) neonatal viremia following placental infection. The neonate is studied clinically, through imaging, and followed up. The neonate presented with neurological manifestations, similar to those described in adult patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
