

D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: a case control study
- PMID: 32665858
- PMCID: PMC7348129
- DOI: 10.1186/s40560-020-00466-z
D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: a case control study
Abstract
Background: Over 5,488,000 cases of coronavirus disease-19 (COVID-19) have been reported since December 2019. We aim to explore risk factors associated with mortality in COVID-19 patients and assess the use of D-dimer as a biomarker for disease severity and clinical outcome.
Methods: We retrospectively analyzed the clinical, laboratory, and radiological characteristics of 248 consecutive cases of COVID-19 in Renmin Hospital of Wuhan University, Wuhan, China from January 28 to March 08, 2020. Univariable and multivariable logistic regression methods were used to explore risk factors associated with in-hospital mortality. Correlations of D-dimer upon admission with disease severity and in-hospital mortality were analyzed. Receiver operating characteristic curve was used to determine the optimal cutoff level for D-dimer that discriminated those survivors versus non-survivors during hospitalization.
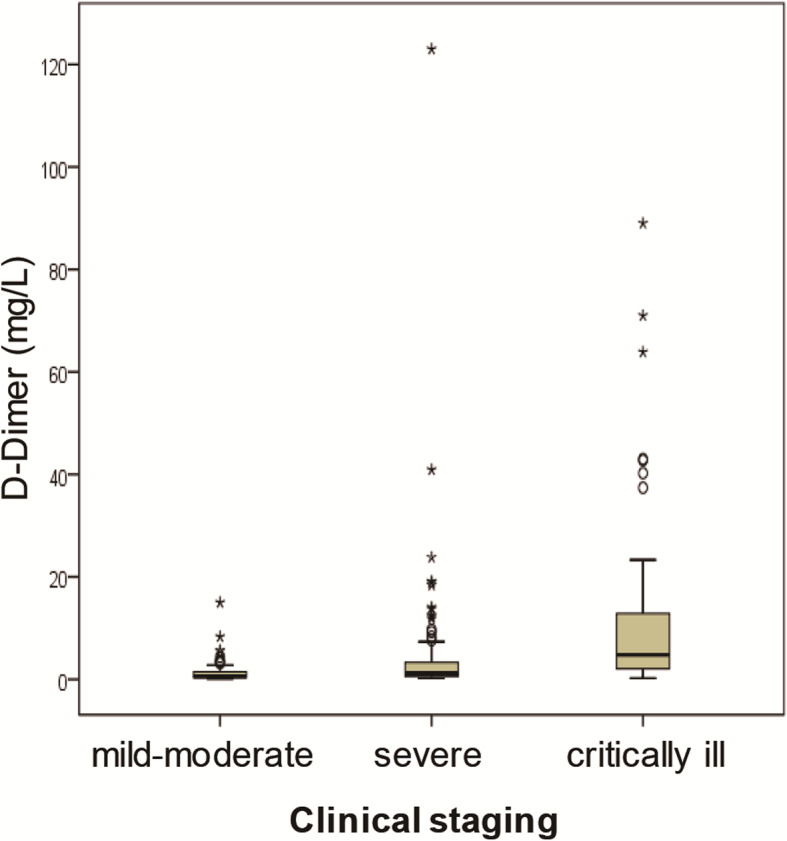
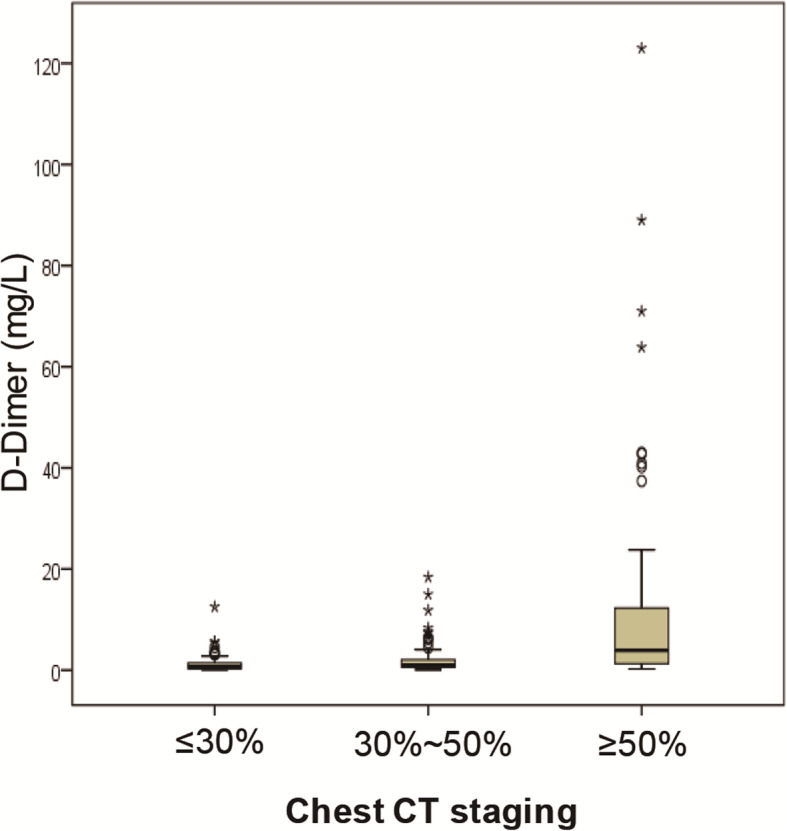
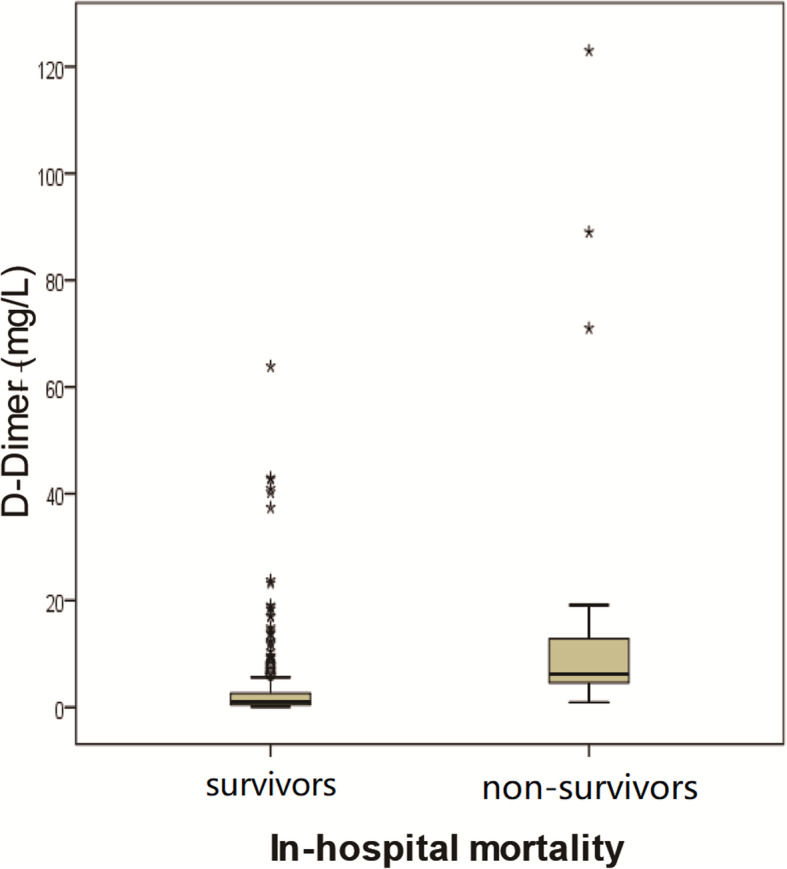
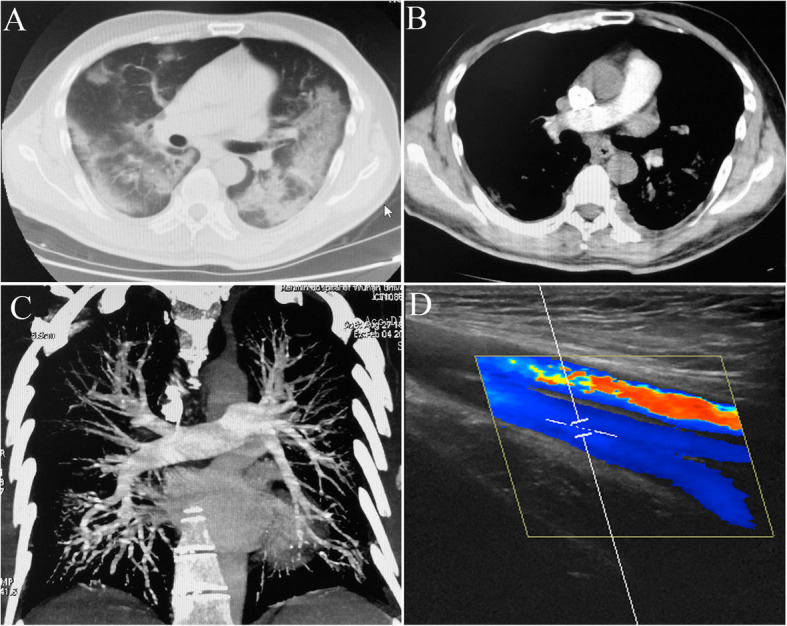
Results: Multivariable regression that showed D-dimer > 2.0 mg/L at admission was the only variable associated with increased odds of mortality [OR 10.17 (95% CI 1.10-94.38), P = 0.041]. D-dimer elevation (≥ 0.50 mg/L) was seen in 74.6% (185/248) of the patients. Pulmonary embolism and deep vein thrombosis were ruled out in patients with high probability of thrombosis. D-dimer levels significantly increased with increasing severity of COVID-19 as determined by clinical staging (Kendall's tau-b = 0.374, P = 0.000) and chest CT staging (Kendall's tau-b = 0.378, P = 0.000). In-hospital mortality rate was 6.9%. Median D-dimer level in non-survivors (n = 17) was significantly higher than in survivors (n = 231) [6.21 (3.79-16.01) mg/L versus 1.02 (0.47-2.66) mg/L, P = 0.000]. D-dimer level of > 2.14 mg/L predicted in-hospital mortality with a sensitivity of 88.2% and specificity of 71.3% (AUC 0.85; 95% CI = 0.77-0.92).
Conclusions: D-dimer is commonly elevated in patients with COVID-19. D-dimer levels correlate with disease severity and are a reliable prognostic marker for in-hospital mortality in patients admitted for COVID-19.
Keywords: Biomarker; Coronavirus disease-19; D-dimer; Mortality; Severity.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests in this section.
Figures

References
-
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi: 10.1016/S0140-6736(20)30211-7. - DOI - PMC - PubMed
-
- Coronavirus disease (COVID-19) Situation Report-128. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... (Accessed 28 May 2020).
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
