

Machine learning to assist clinical decision-making during the COVID-19 pandemic
- PMID: 32665967
- PMCID: PMC7347420
- DOI: 10.1186/s42234-020-00050-8
Machine learning to assist clinical decision-making during the COVID-19 pandemic
Abstract
Background: The number of cases from the coronavirus disease 2019 (COVID-19) global pandemic has overwhelmed existing medical facilities and forced clinicians, patients, and families to make pivotal decisions with limited time and information.
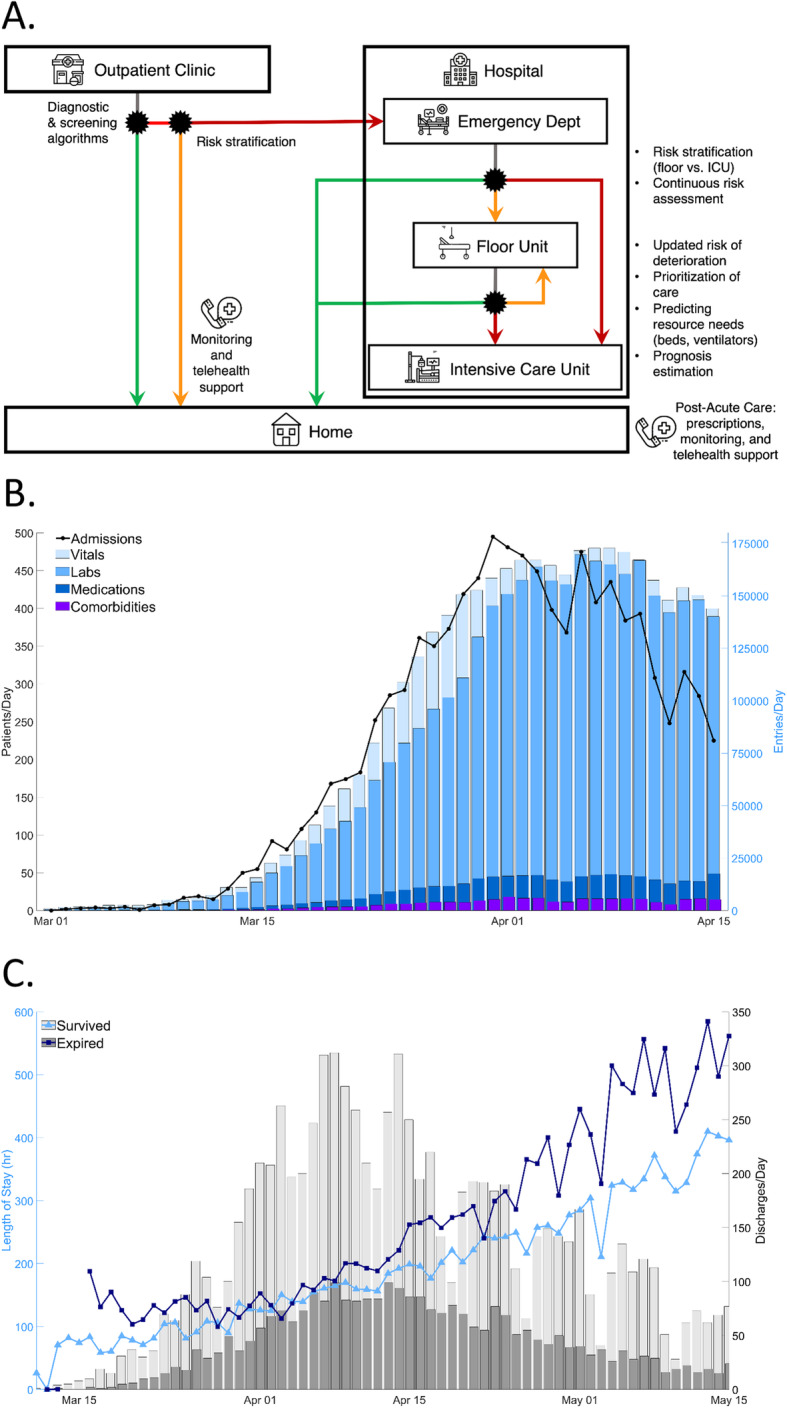
Main body: While machine learning (ML) methods have been previously used to augment clinical decisions, there is now a demand for "Emergency ML." Throughout the patient care pathway, there are opportunities for ML-supported decisions based on collected vitals, laboratory results, medication orders, and comorbidities. With rapidly growing datasets, there also remain important considerations when developing and validating ML models.
Conclusion: This perspective highlights the utility of evidence-based prediction tools in a number of clinical settings, and how similar models can be deployed during the COVID-19 pandemic to guide hospital frontlines and healthcare administrators to make informed decisions about patient care and managing hospital volume.
Keywords: Artificial intelligence (AI); Clinical decision-making; Coronavirus disease 19 (COVID-19); Healthcare; Machine learning (ML).
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
References
-
- Bai X, Fang C, Zhou Y, Bai S, Liu Z, Chen Q, Xu Y, Xia T, Gong S, Xie X, et al. Predicting COVID-19 malignant progression with AI techniques. medRxiv. 2020.03.20.20037325.
-
- Batista AFM, Miraglia JL, Donato THR, Chiavegatto Filho ADP. COVID-19 diagnosis prediction in emergency care patients: a machine learning approach. medRxiv. 2020.04.04.20052092.
Grants and funding
LinkOut - more resources
Full Text Sources