

Metabolic inflammation in heart failure with preserved ejection fraction
- PMID: 32666082
- PMCID: PMC8599724
- DOI: 10.1093/cvr/cvaa217
Metabolic inflammation in heart failure with preserved ejection fraction
Abstract
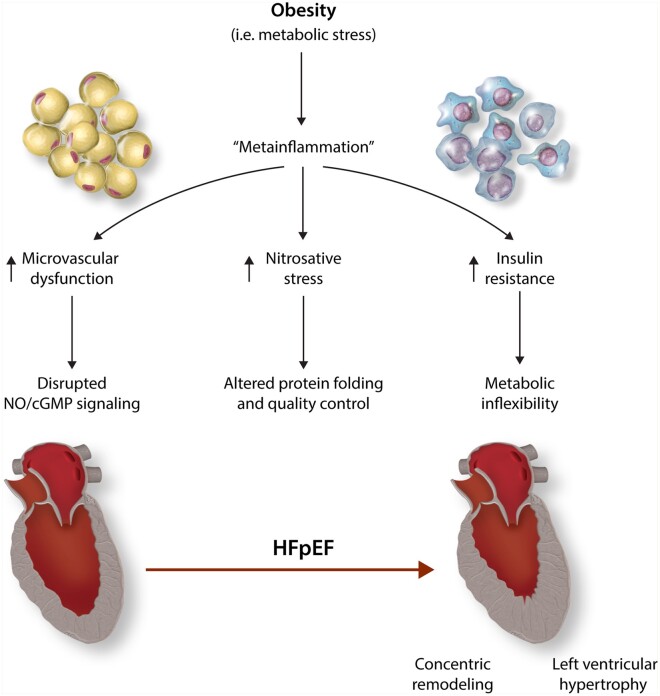
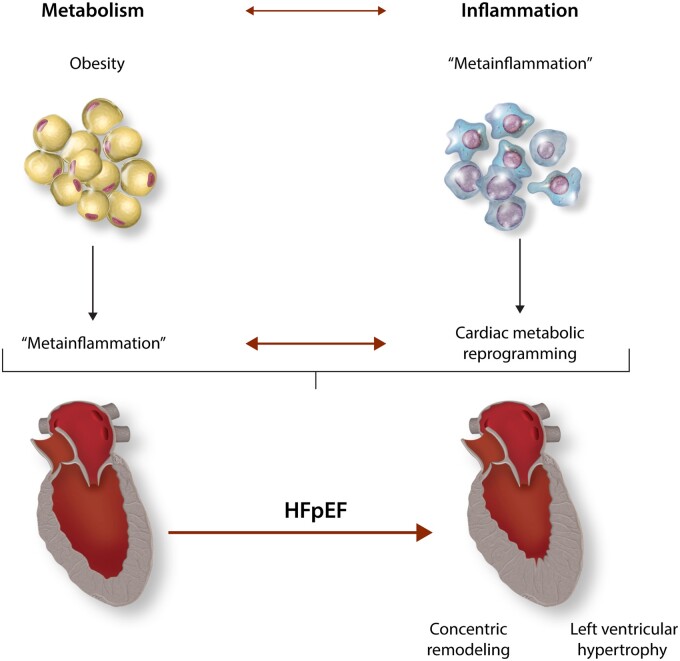
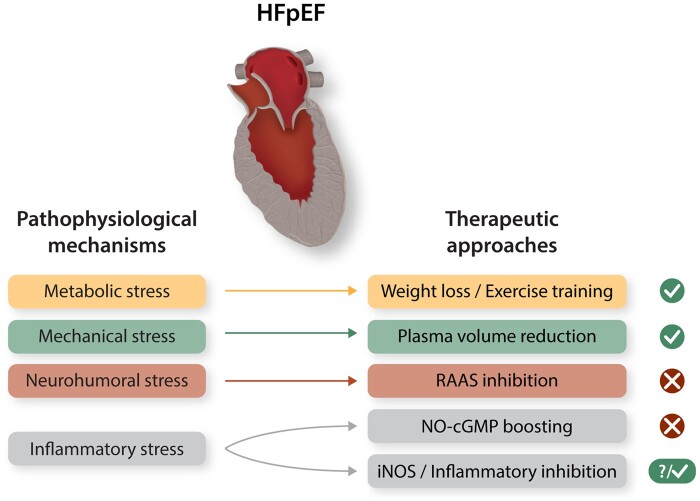
One in 10 persons in the world aged 40 years and older will develop the syndrome of HFpEF (heart failure with preserved ejection fraction), the most common form of chronic cardiovascular disease for which no effective therapies are currently available. Metabolic disturbance and inflammatory burden contribute importantly to HFpEF pathogenesis. The interplay within these two biological processes is complex; indeed, it is now becoming clear that the notion of metabolic inflammation-metainflammation-must be considered central to HFpEF pathophysiology. Inflammation and metabolism interact over the course of syndrome progression, and likely impact HFpEF treatment and prevention. Here, we discuss evidence in support of a causal, mechanistic role of metainflammation in shaping HFpEF, proposing a framework in which metabolic comorbidities profoundly impact cardiac metabolism and inflammatory pathways in the syndrome.
Keywords: HFpEF; Immunity; Inflammation; Metabolism; Obesity.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Fact Sheet on Obesity and Overweight. World Health Organization. www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (1 April....
-
- Kitzman DW, Lam C.. Obese heart failure with preserved ejection fraction phenotype: from pariah to central player. Circulation 2017;136:20–23. - PubMed
-
- Packer M. Do most patients with obesity or type 2 diabetes, and atrial fibrillation, also have undiagnosed heart failure? A critical conceptual framework for understanding mechanisms and improving diagnosis and treatment. Eur J Heart Fail 2020;22:214–227. - PubMed
-
- Pandey A, Patel KV, Vaduganathan M, Sarma S, Haykowsky MJ, Berry JD, Lavie CJ.. Physical activity, fitness, and obesity in heart failure with preserved ejection fraction. JACC Heart Fail 2018;6:975–982. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
