

The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-analysis
- PMID: 32666247
- PMCID: PMC7497464
- DOI: 10.1007/s40279-020-01317-5
The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-analysis
Abstract
Background: Oral contraceptive pills (OCPs) are double agents, which downregulate endogenous concentrations of oestradiol and progesterone whilst simultaneously providing daily supplementation of exogenous oestrogen and progestin during the OCP-taking days. This altered hormonal milieu differs significantly from that of eumenorrheic women and might impact exercise performance, due to changes in ovarian hormone-mediated physiological processes.
Objective: To explore the effects of OCPs on exercise performance in women and to provide evidence-based performance recommendations to users.
Methods: This review complied with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A between-group analysis was performed, wherein performance of OCP users was compared with naturally menstruating women, and a within-group analysis was conducted, wherein performance during OCP consumption was compared with OCP withdrawal. For the between-group analysis, women were phase matched in two ways: (1) OCP withdrawal versus the early follicular phase of the menstrual cycle and (2) OCP consumption versus all phases of the menstrual cycle except for the early follicular phase. Study quality was assessed using a modified Downs and Black Checklist and a strategy based on the recommendations of the Grading of Recommendations Assessment Development and Evaluation working group. All meta-analyses were conducted within a Bayesian framework to facilitate probabilistic interpretations.
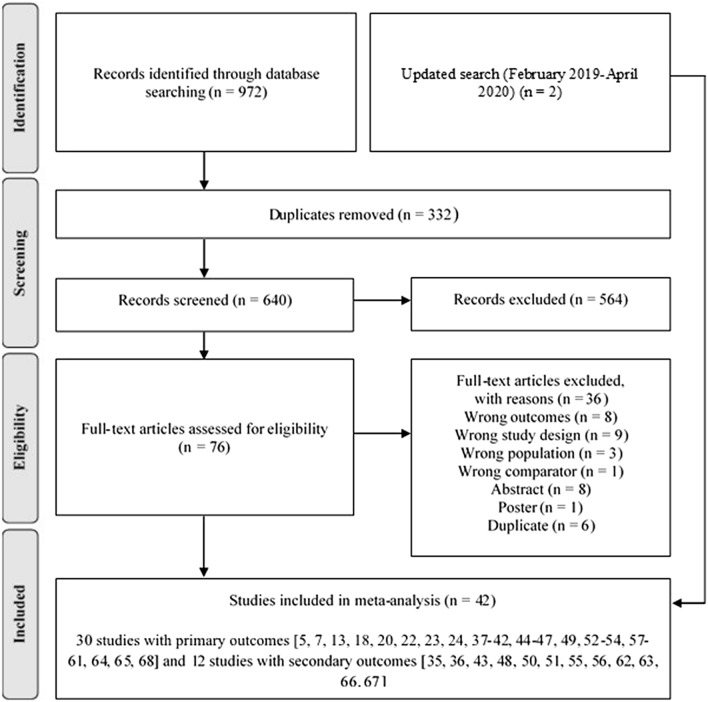
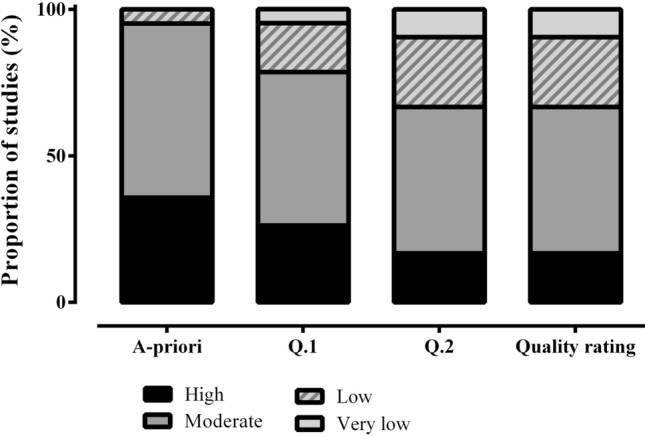
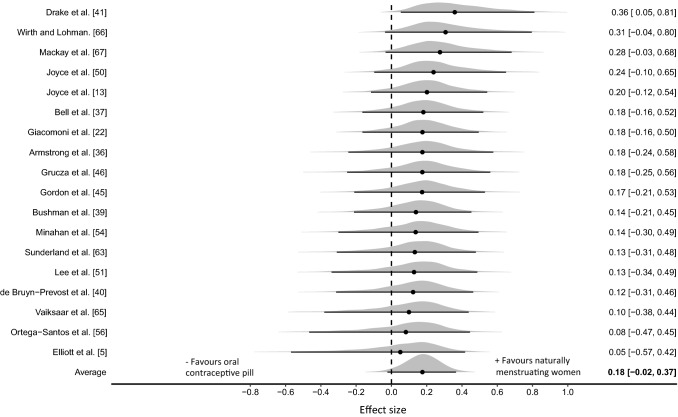
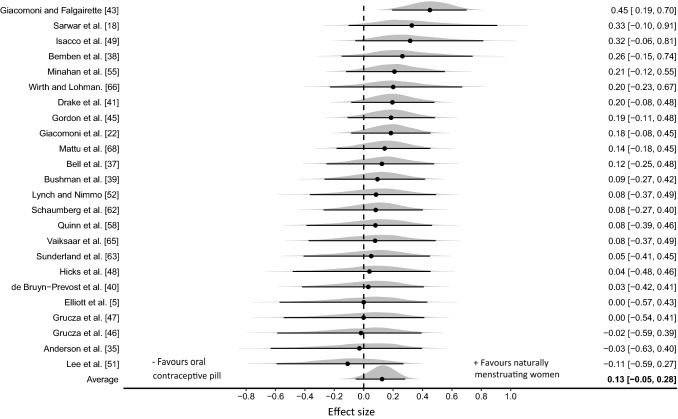
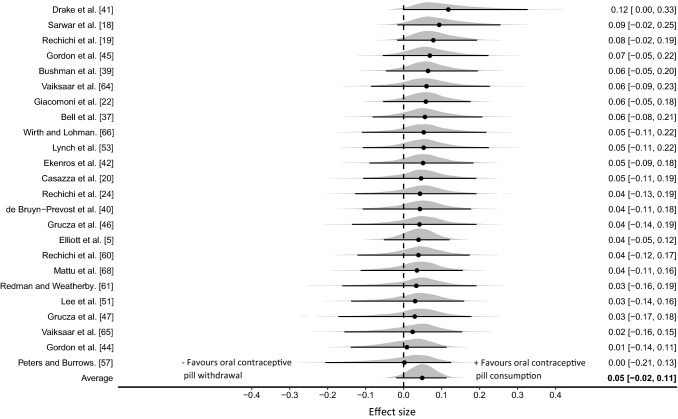
Results: 42 studies and 590 participants were included. Most studies (83%) were graded as moderate, low or very low quality, with 17% achieving high quality. For the between-group meta-analysis comparing OCP users with naturally menstruating women, posterior estimates of the pooled effect were used to calculate the probability of at least a small effect (d ≥ 0.2). Across the two between-group comparison methods, the probability of a small effect on performance favouring habitual OCP users was effectually zero (p < 0.001). In contrast, the probability of a small effect on performance favouring naturally menstruating women was moderate under comparison method (1) (d ≥ 0.2; p = 0.40) and small under comparison method (2) (d ≥ 0.2; p = 0.19). Relatively large between-study variance was identified for both between-group comparisons ([Formula: see text]0.5 = 0.16 [95% credible interval (CrI) 0.01-0.44] and [Formula: see text]0.5 = 0.22 [95% CrI 0.06-0.45]). For the within-group analysis comparing OCP consumption with withdrawal, posterior estimates of the pooled effect size identified almost zero probability of a small effect on performance in either direction (d ≥ 0.2; p ≤ 0.001).
Conclusions: OCP use might result in slightly inferior exercise performance on average when compared to naturally menstruating women, although any group-level effect is most likely to be trivial. Practically, as effects tended to be trivial and variable across studies, the current evidence does not warrant general guidance on OCP use compared with non-use. Therefore, when exercise performance is a priority, an individualised approach might be more appropriate. The analysis also indicated that exercise performance was consistent across the OCP cycle.
Conflict of interest statement
Kirsty Elliott-Sale, Kirsty Hicks, Kelly McNulty, Paul Ansdell, Stuart Goodall, Kevin Thomas, Paul Swinton and Eimear Dolan declare that they have no potential conflicts of interest with the content of this article.
Figures
Comment in
-
Reply to: Comment on: "The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis" and "The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-analysis".Sports Med. 2021 May;51(5):1111-1113. doi: 10.1007/s40279-020-01383-9. Sports Med. 2021. PMID: 33332009 No abstract available.
-
Comment on: "The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis" and "The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-analysis".Sports Med. 2021 May;51(5):1107-1109. doi: 10.1007/s40279-020-01384-8. Epub 2020 Dec 17. Sports Med. 2021. PMID: 33332010 No abstract available.
References
-
- Kinsley C, Bardi M, Neigh GN, Lambert K. Chapter 2—chromosomal and endocrinological origins of sex. In: Neigh GN, Mitzelfelt MM, editors. Sex differences in physiology. New York: Academic Press; 2016. pp. 5–15.
-
- Reilly T. The menstrual cycle and human performance: an overview. Biol Rhythm Res. 2000;31(1):29–40. - PubMed
-
- Martin D, Sale C, Cooper SB, Elliott-Sale KJ. Period prevalence and perceived side effects of hormonal contraceptive use and the menstrual cycle in elite athletes. Int J Sports Physiol Perform. 2018;13(7):926–932. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
