

Phase Ib/II Study of Biweekly TAS-102 in Combination with Bevacizumab for Patients with Metastatic Colorectal Cancer Refractory to Standard Therapies (BiTS Study)
- PMID: 32666647
- PMCID: PMC8108052
- DOI: 10.1634/theoncologist.2020-0643
Phase Ib/II Study of Biweekly TAS-102 in Combination with Bevacizumab for Patients with Metastatic Colorectal Cancer Refractory to Standard Therapies (BiTS Study)
Erratum in
-
Correction to: Phase Ib/II Study of Biweekly TAS-102 in Combination with Bevacizumab for Patients with Metastatic Colorectal Cancer Refractory to Standard Therapies (BiTS Study).Oncologist. 2025 May 8;30(5):oyaf119. doi: 10.1093/oncolo/oyaf119. Oncologist. 2025. PMID: 40445170 Free PMC article. No abstract available.
Abstract
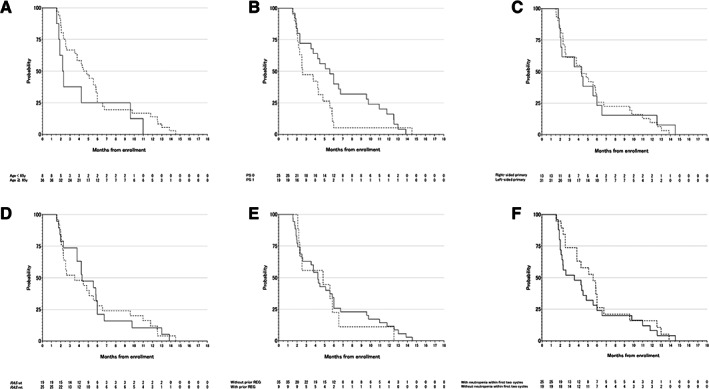
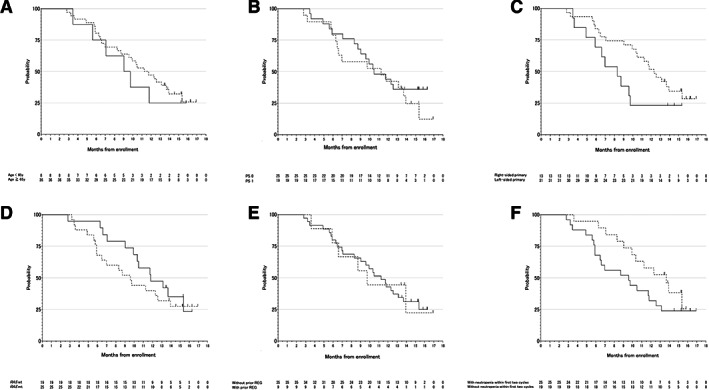
Lessons learned: A biweekly TAS-102 plus BEV schedule in patients with heavily pretreated mCRC showed equivalent efficacy with less toxicity compared with the current schedule of TAS-102 plus BEV combination. Biweekly TAS-102 plus BEV combination could reduce unnecessary dose reduction of TAS-102, maintain higher doses, and possibly be effective even in cases without chemotherapy-induced neutropenia (CIN). The prespecified subgroup analysis of this study showed an obvious association between CIN within the first two cycles and prognosis of biweekly TAS-102 plus BEV.
Background: TAS-102 (trifluridine/tipiracil) plus bevacizumab (BEV) combination therapy has shown promising activity in patients with metastatic colorectal cancer (mCRC). However, the previously reported dose and schedule for the TAS-102 (70 mg/m2 /day on days 1-5 and 8-12, every 4 weeks) plus BEV (5 mg/kg on day 1, every 2 weeks) regimen is complicated by severe hematological toxicities and difficult administration schedules. Here, we evaluated the efficacy and safety of a more convenient biweekly TAS-102 plus BEV combination.
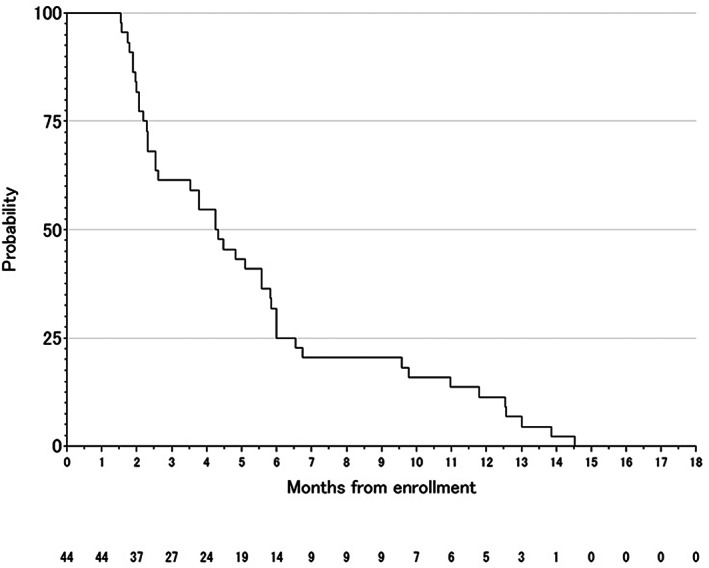
Methods: Patients with mCRC who were refractory or intolerant to standard chemotherapies were enrolled. Patients received biweekly TAS-102 (twice daily on days 1-5, every 2 weeks) with BEV (5mg/kg on day 1, every 2 weeks). The primary endpoint was progression-free survival rate at 16 weeks (16-w PFS rate).
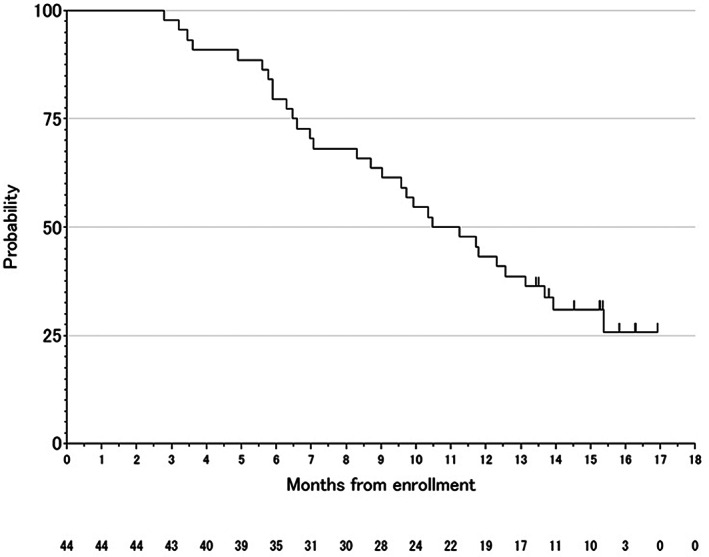
Results: From October 2017 to January 2018, 46 patients were enrolled. The recommended phase II dose was determined to be TAS-102 (70 mg/m2 /day). Of the 44 eligible patients, the 16-w PFS rate was 40.9% (95% confidence interval, 26.3%-56.8%), and the null hypothesis was rejected (p < .0001). Median progression-free survival (PFS) and overall survival were 4.29 months and 10.86 months, respectively. Disease control rate was 59.1%. Common grade 3 or higher adverse events were hypertension (40.9%), neutropenia (15.9%), and leucopenia (15.9%).
Conclusion: Biweekly TAS-102 plus BEV showed promising antitumor activity with safety.
© 2020 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Figures
References
-
- Yoshino T, Mizunuma N, Yamazaki K et al. TAS‐102 monotherapy for pretreated metastatic colorectal cancer: A double‐blind, randomised, placebo‐controlled phase 2 trial. Lancet Oncol 2012;13:993–1001. - PubMed
-
- Mayer RJ, Van Cutsem E, Falcone A et al. Randomized trial of TAS‐102 for refractory metastatic colorectal cancer. N Engl J Med 2015;372:1909–1919. - PubMed
-
- Kuboki Y, Nishina T, Shinozaki E et al. TAS‐102 plus bevacizumab for patients with metastatic colorectal cancer refractory to standard therapies (C‐TASK FORCE): An investigator‐initiated, open‐label, single‐arm, multicentre, phase 1/2 study. Lancet Oncol 2017;18:1172–1181. - PubMed
-
- Pfeiffer P, Yilmaz M, Moller S et al. TAS‐102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: An investigator‐initiated, open‐label, randomised, phase 2 trial. Lancet Oncol 2020;21:412–420. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
