

Shoulder-Pacemaker Treatment Concept for Posterior Positional Functional Shoulder Instability: A Prospective Clinical Trial
- PMID: 32667266
- PMCID: PMC7364790
- DOI: 10.1177/0363546520933841
Shoulder-Pacemaker Treatment Concept for Posterior Positional Functional Shoulder Instability: A Prospective Clinical Trial
Abstract
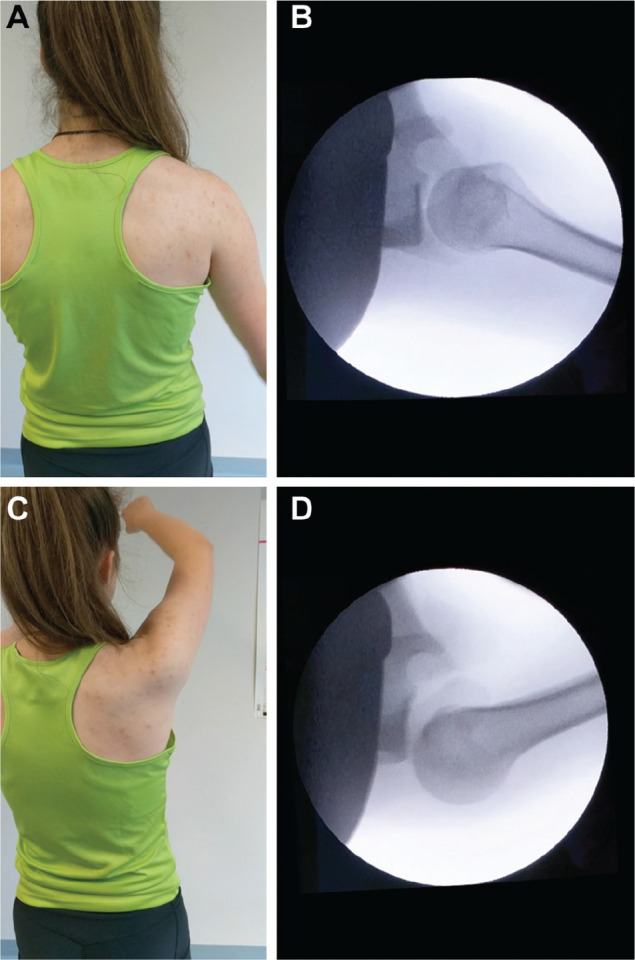
Background: Pathological muscle activation patterns of the external rotators and periscapular muscles can result in posterior positional functional shoulder instability (PP-FSI). In several patients, physical therapy and surgical treatment are not successful.
Purpose: The shoulder-pacemaker treatment concept was evaluated prospectively in patients with PP-FSI and previously failed conventional therapy attempt.
Study design: Case series; Level of evidence, 4.
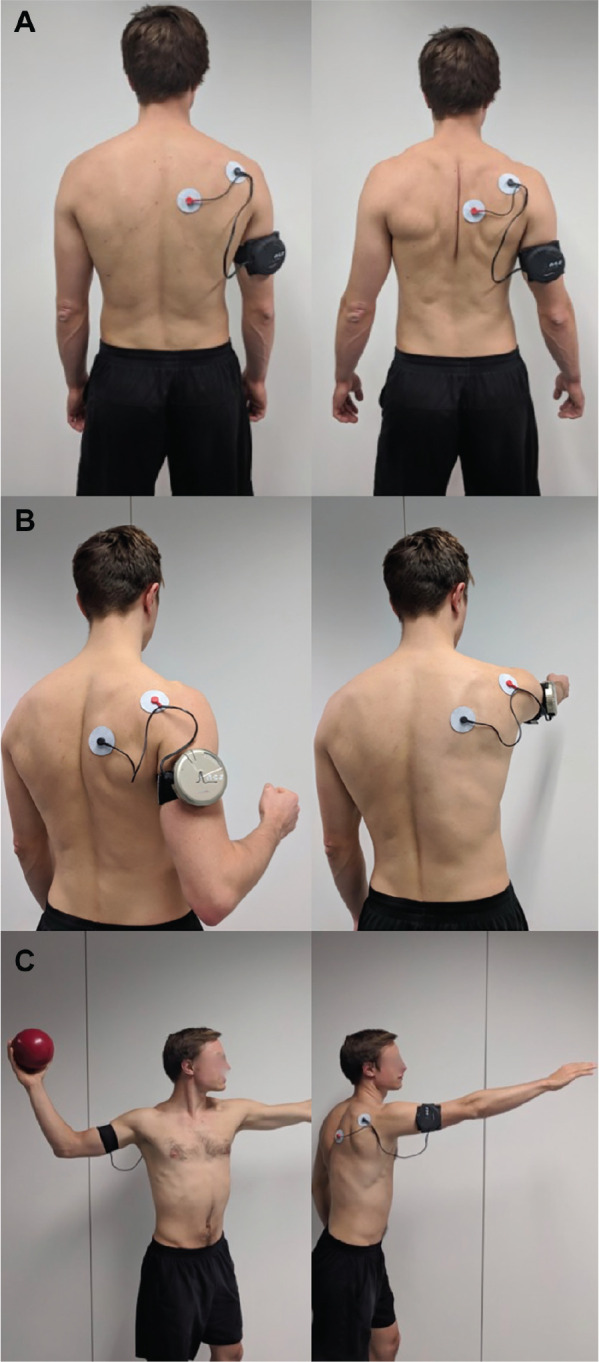
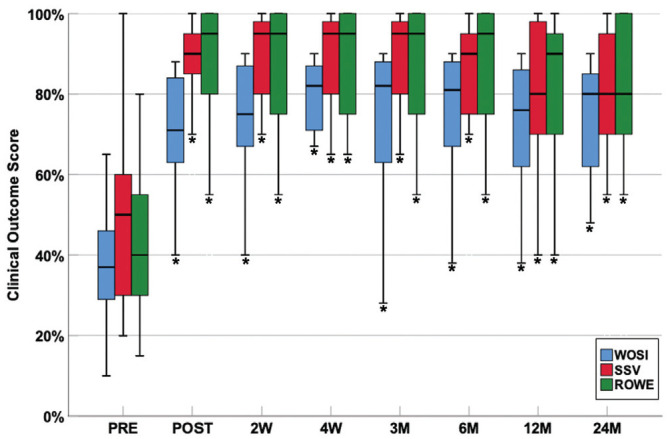
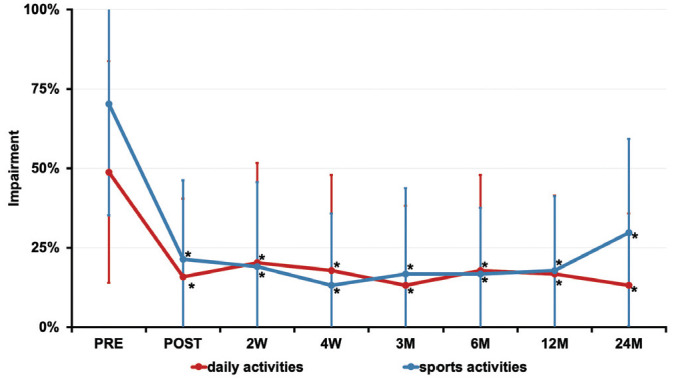
Methods: A negative selection of 24 consecutive cases of noncontrollable PP-FSI in 16 patients with previously failed conventional therapy were included in this prospective study. The shoulder-pacemaker treatment consisted of an electrical muscle stimulation-based therapy protocol with 9 to 18 one-hour treatment sessions. Two patients were excluded because of nonadherence to the training schedule, leaving a final study cohort of 21 cases in 14 patients. Follow-up included assessment of clinical function, impairment during daily activities and sports, satisfaction, Western Ontario Shoulder Instability Index (WOSI), Rowe score, and Subjective Shoulder Value at 0 weeks, 2 weeks, 4 weeks, 3 months, 6 months, 12 months, and 24 months after intervention.
Results: WOSI, Subjective Shoulder Value, and Rowe score showed a highly significant improvement at all time points of follow-up (P < .001). Young age (P = .005), low weight (P = .019), shoulder activity level (P = .003), unilateral affliction (P = .046), and higher baseline WOSI score (P = .04) were associated with a better treatment effect. Cases with increased glenoid retroversion, posterior scapulohumeral decentering, and dysplastic bony glenoid shape showed a trend toward shorter treatment effect duration. No complications during the intervention or follow-up period were observed.
Conclusion: The shoulder-pacemaker therapy concept is an effective treatment with rapid improvement and sustained outcome over the course of 2 years in patients with noncontrollable PP-FSI with previously failed conventional treatment. Young and more athletic patients with lower weight and unilateral pathology respond best to the treatment.
Keywords: EMS treatment; functional shoulder instability; posterior positional functional shoulder instability; posterior shoulder instability; rehabilitation; shoulder-pacemaker; voluntary shoulder instability.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Material support was provided by NCS Lab and DJO Global. P.M. has the potential to receive royalties from NCS Lab. H.V.-V. was formerly employed by DJO Global. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Alexander CM. Altered control of the trapezius muscle in subjects with non-traumatic shoulder instability. Clin Neurophysiol. 2007;118(12):2664-2671. - PubMed
-
- Barden JM, Balyk R, Raso VJ, Moreau M, Bagnall K. Atypical shoulder muscle activation in multidirectional instability. Clin Neurophysiol. 2005;116(8):1846-1857. - PubMed
-
- Baum J, Larsson LG. Hypermobility syndrome—new diagnostic criteria. J Rheumatol. 2000;27(7):1585-1586. - PubMed
-
- Beall MS, Jr, Diefenbach G, Allen A. Electromyographic biofeedback in the treatment of voluntary posterior instability of the shoulder. Am J Sports Med. 1987;15(2):175-178. - PubMed
-
- Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML. Posterior glenohumeral subluxation: active and passive stabilization in a biomechanical model. J Bone Joint Surg Am. 1997;79(3):433-440. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
