

Incubator-based Sound Attenuation: Active Noise Control In A Simulated Clinical Environment
- PMID: 32667931
- PMCID: PMC7363066
- DOI: 10.1371/journal.pone.0235287
Incubator-based Sound Attenuation: Active Noise Control In A Simulated Clinical Environment
Abstract
Objective: Noise in the neonatal intensive care unit can be detrimental to the health of the hospitalized infant. Means of reducing that noise include staff training, warning lights, and ear coverings, all of which have had limited success. Single family rooms, while an improvement, also expose the hospitalized infant to the same device alarms and mechanical noises found in open bay units.
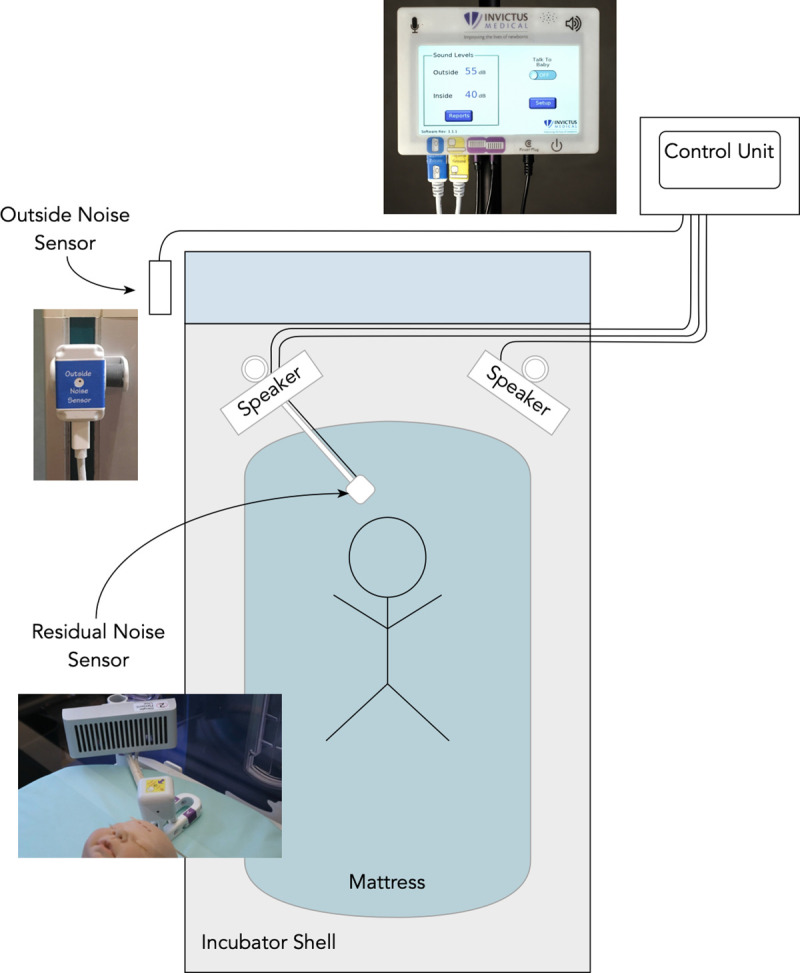
Methods: We evaluated a non-contact incubator-based active noise control device (Neoasis™, Invictus Medical, San Antonio, Texas) in a simulated neonatal intensive care unit (NICU) setting to determine whether it could effectively reduce the noise exposure of infants within an incubator. In the NICU simulation center, we generated a series of clinically appropriate sound sequences with bedside medical devices such as a patient monitor and fluid infusion devices, hospital air handling systems, and device mechanical sounds. A microphone-equipped infant mannequin was oriented within an incubator. Measurements were made with the microphones with the Neoasis™ deactivated and activated.
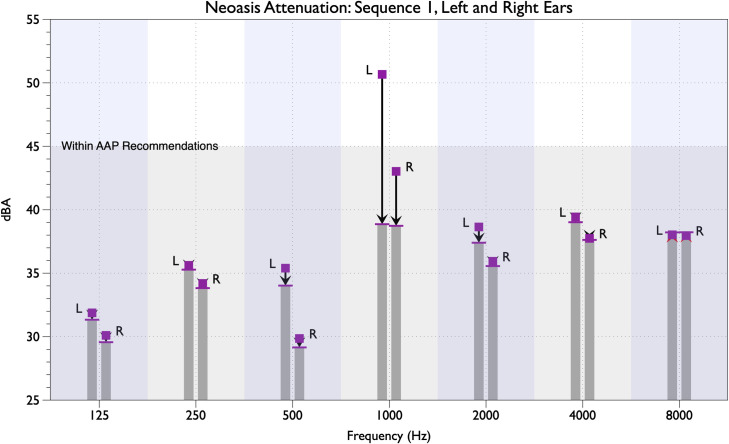
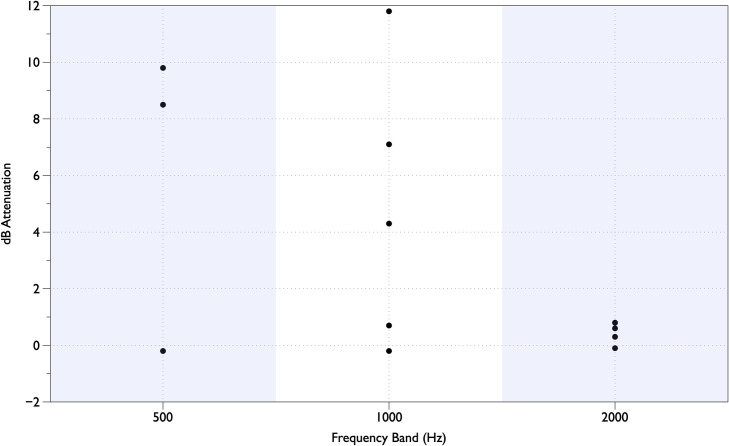
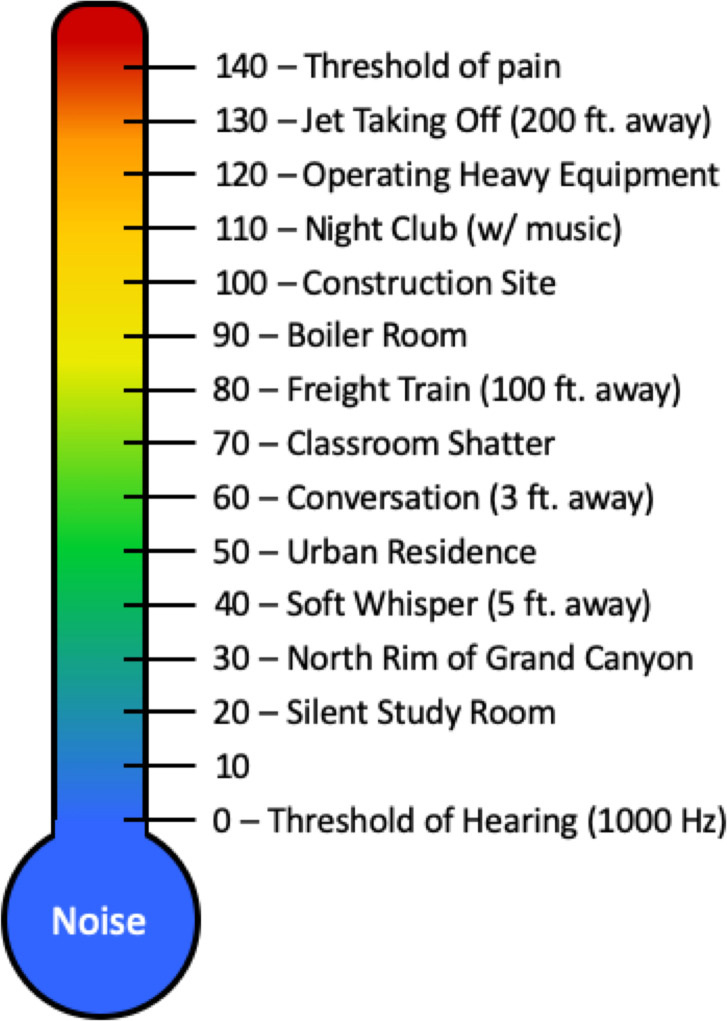
Results: The active noise control device decreased sound pressure levels for certain alarm sounds by as much as 14.4 dB (a 5.2-fold reduction in sound pressure) at the alarm tone's primary frequency. Frequencies below the 2 kHz octave band were more effectively attenuated than frequencies at or above the 2 kHz octave band. Background noise levels below 40 dBA were essentially not impacted by the active noise control device.
Conclusions: The active noise control device further reduces noise inside infant incubators. Device safety and potential health benefits of the quieter environment should be verified in a clinical setting.
Conflict of interest statement
The authors have read the journal's policy and have the following competing interests: GH is a paid employee, board member, and shareholder of Invictus Medical, and is a named inventor of patent applications assigned to the company manufacturing the equipment used in this study. LD is an employee and shareholder of the company manufacturing the equipment used in this study, and is also a named inventor of patent applications assigned to the company manufacturing the equipment used in this study. The authors would like to declare the following patents/patent applications associated with this research: US10410619, Active Noise Control Microphone Array. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures

Similar articles
-
Incubator-based active noise control device: comparison to ear covers and noise reduction zone quantification.Pediatr Res. 2023 Nov;94(5):1817-1823. doi: 10.1038/s41390-023-02708-w. Epub 2023 Jul 6. Pediatr Res. 2023. PMID: 37414919 Free PMC article.
-
Neonatal incubators: a toxic sound environment for the preterm infant?*.Pediatr Crit Care Med. 2012 Nov;13(6):685-9. doi: 10.1097/PCC.0b013e31824ea2b7. Pediatr Crit Care Med. 2012. PMID: 22791088
-
Noise and Critical Sound Levels During Non-Invasive Ventilation of a Preterm Infant in the Incubator.Klin Padiatr. 2023 Jul;235(4):228-234. doi: 10.1055/a-1906-0960. Epub 2022 Sep 15. Klin Padiatr. 2023. PMID: 36108643 English.
-
NICU noise and the preterm infant.Neonatal Netw. 2009 May-Jun;28(3):165-73. doi: 10.1891/0730-0832.28.3.165. Neonatal Netw. 2009. PMID: 19451078 Review.
-
The infant incubator in the neonatal intensive care unit: unresolved issues and future developments.J Perinat Med. 2009;37(6):587-98. doi: 10.1515/JPM.2009.109. J Perinat Med. 2009. PMID: 19591569 Review.
Cited by
-
Concept and considerations of a medical device: the active noise cancelling incubator.Front Pediatr. 2023 Jul 3;11:1187815. doi: 10.3389/fped.2023.1187815. eCollection 2023. Front Pediatr. 2023. PMID: 37465419 Free PMC article.
-
Noise in ICUs: Review and Detailed Analysis of Long-Term SPL Monitoring in ICUs in Northern Spain.Sensors (Basel). 2022 Nov 22;22(23):9038. doi: 10.3390/s22239038. Sensors (Basel). 2022. PMID: 36501740 Free PMC article. Review.
-
Newborn Incubators Do Not Protect from High Noise Levels in the Neonatal Intensive Care Unit and Are Relevant Noise Sources by Themselves.Children (Basel). 2021 Aug 16;8(8):704. doi: 10.3390/children8080704. Children (Basel). 2021. PMID: 34438595 Free PMC article.
-
Sensory Stimulation in the NICU Environment: Devices, Systems, and Procedures to Protect and Stimulate Premature Babies.Children (Basel). 2021 Apr 25;8(5):334. doi: 10.3390/children8050334. Children (Basel). 2021. PMID: 33923031 Free PMC article. Review.
-
Incubator-based active noise control device: comparison to ear covers and noise reduction zone quantification.Pediatr Res. 2023 Nov;94(5):1817-1823. doi: 10.1038/s41390-023-02708-w. Epub 2023 Jul 6. Pediatr Res. 2023. PMID: 37414919 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
