

SARS-CoV-2 (COVID-19) and cystic fibrosis
- PMID: 32668165
- PMCID: PMC7518058
- DOI: 10.1152/ajplung.00225.2020
SARS-CoV-2 (COVID-19) and cystic fibrosis
Abstract
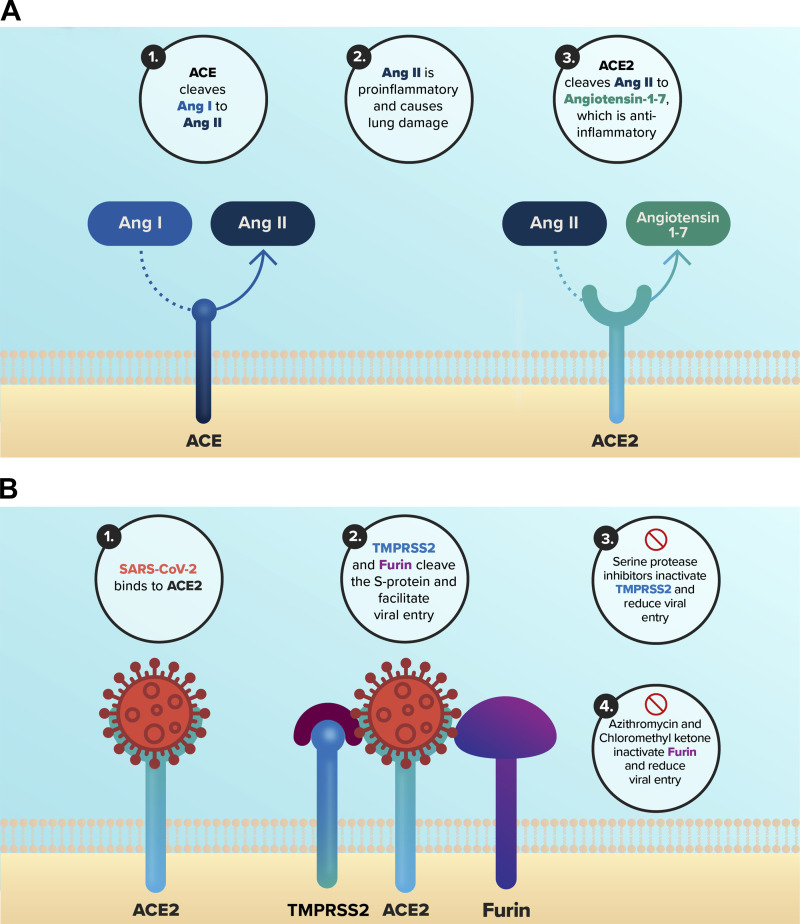
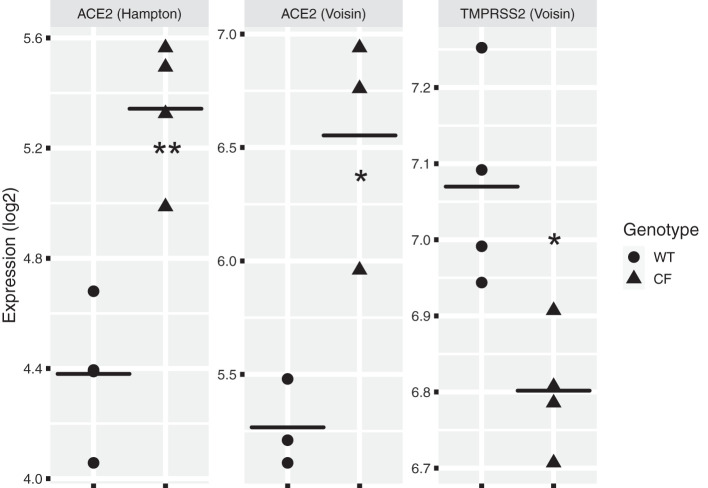
Cystic fibrosis (CF) is a genetic disease caused by mutations in the CFTR gene. Although viral respiratory tract infections are, in general, more severe in patients with CF compared with the general population, a small number of studies indicate that SARS-CoV-2 does not cause a worse infection in CF. This is surprising since comorbidities including preexisting lung disease have been reported to be associated with worse outcomes in SARS-CoV-2 infections. Several recent studies provide insight into why SARS-CoV-2 may not produce more severe outcomes in CF. First, ACE and ACE2, genes that play key roles in SARS-CoV-2 infection, have some variants that are predicted to reduce the severity of SARS-CoV-2 infection. Second, mRNA for ACE2 is elevated and mRNA for TMPRSS2, a serine protease, is decreased in CF airway epithelial cells. Increased ACE2 is predicted to enhance SARS-CoV-2 binding to cells but would increase conversion of angiotensin II, which is proinflammatory, to angiotensin-1-7, which is anti-inflammatory. Thus, increased ACE2 would reduce inflammation and lung damage due to SARS-CoV-2. Moreover, decreased TMPRSS2 would reduce SARS-CoV-2 entry into airway epithelial cells. Second, many CF patients are treated with azithromycin, which suppresses viral infection and lung inflammation and inhibits the activity of furin, a serine protease. Finally, the CF lung contains high levels of serine protease inhibitors including ecotin and SERPINB1, which are predicted to reduce the ability of TMPRSS2 to facilitate SARS-CoV-2 entry into airway epithelial cells. Thus, a variety of factors may mitigate the severity of SARS-CoV-2 in CF.
Keywords: ACE2; COVID-19; SARS-CoV-2; TMPRSS2; cystic fibrosis.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Abassi ZA, Skorecki K, Heyman SN, Kinaneh S, Armaly Z. Covid-19 infection and mortality: a physiologist’s perspective enlightening clinical features and plausible interventional strategies. Am J Physiol Lung Cell Mol Physiol 318: L1020–L1022, 2020. doi:10.1152/ajplung.00097.2020. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous