

Towards Breathing as a Sensing Modality in Depth-Based Activity Recognition
- PMID: 32668594
- PMCID: PMC7412468
- DOI: 10.3390/s20143884
Towards Breathing as a Sensing Modality in Depth-Based Activity Recognition
Abstract
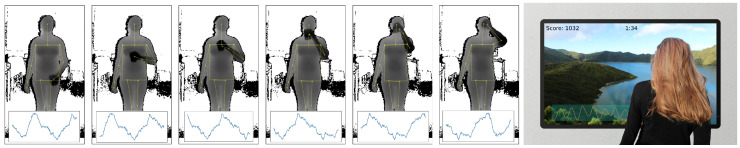
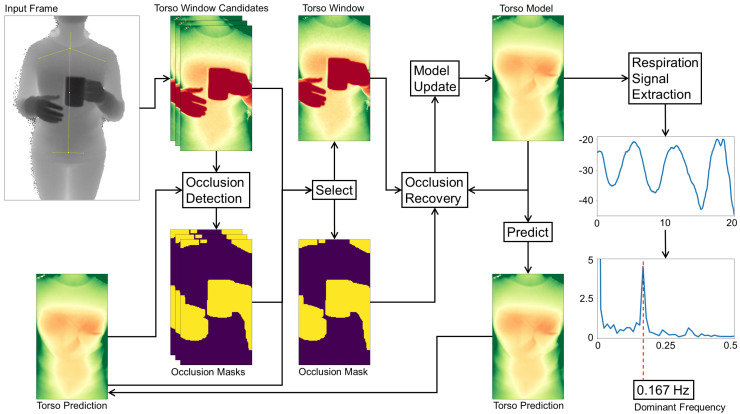
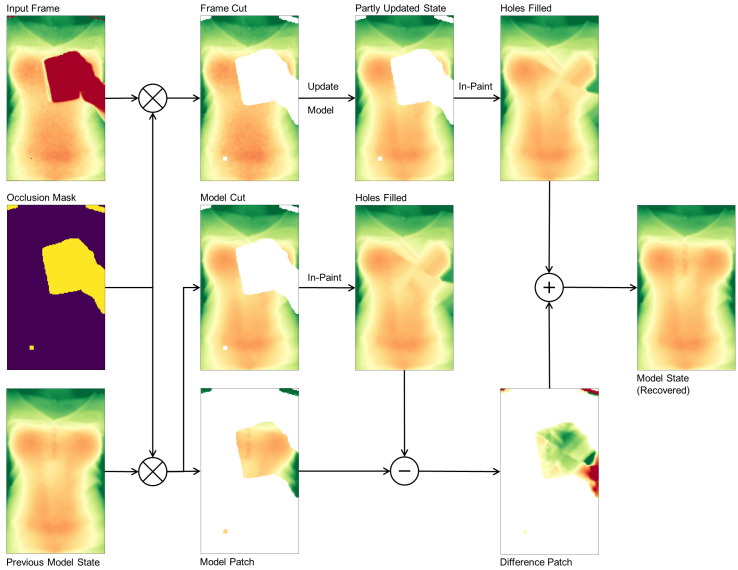
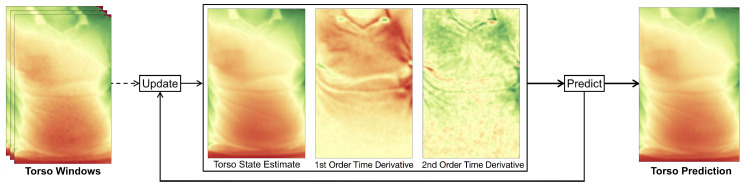
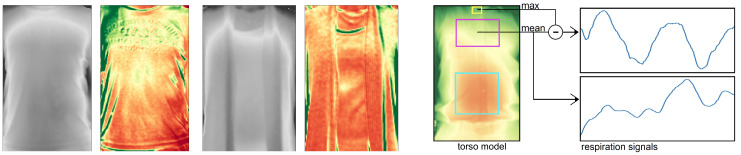
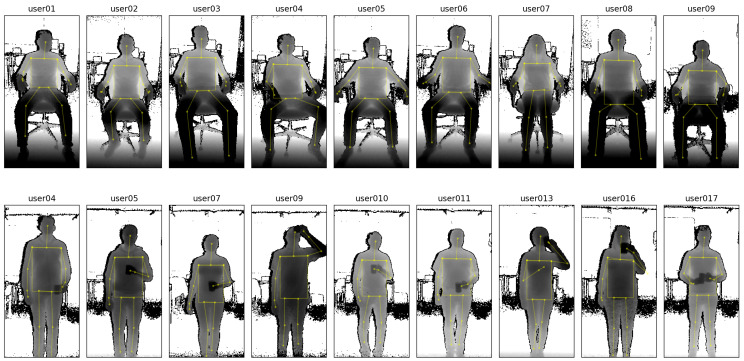
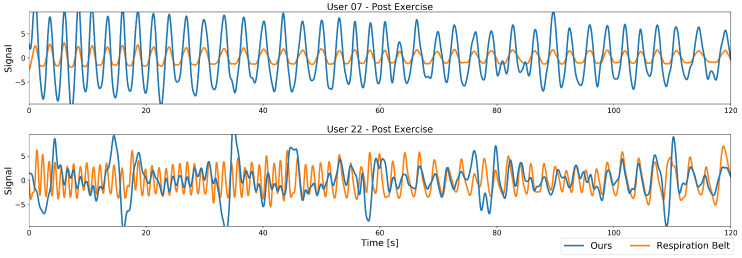
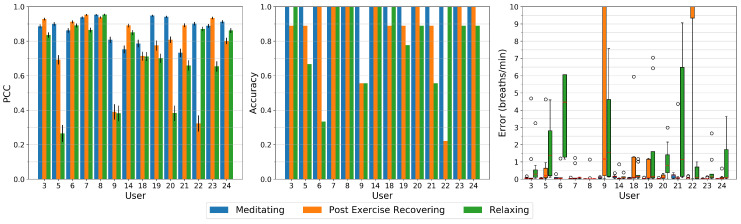
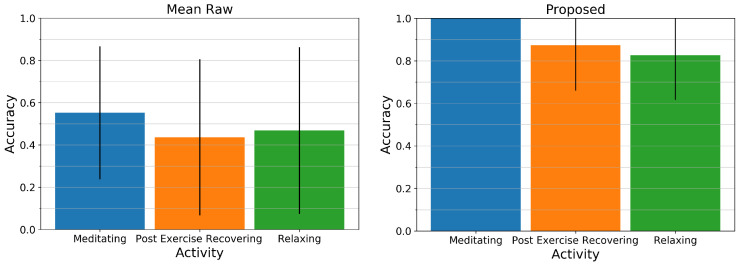
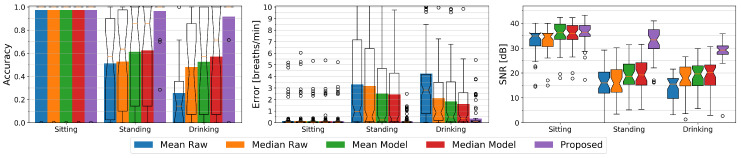
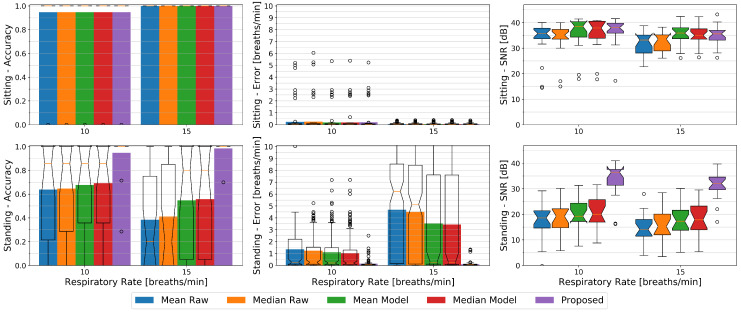
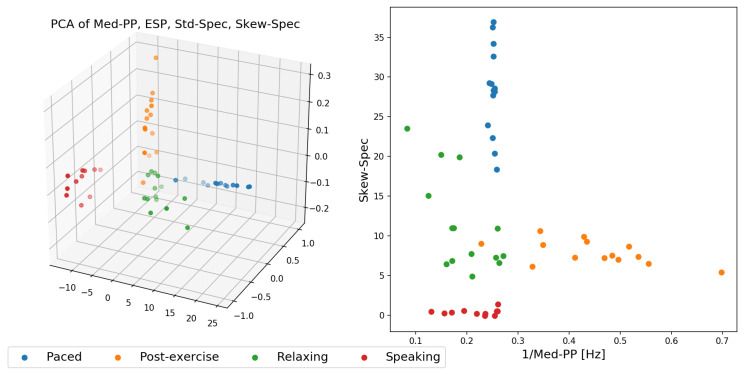
Depth imaging has, through recent technological advances, become ubiquitous as products become smaller, more affordable, and more precise. Depth cameras have also emerged as a promising modality for activity recognition as they allow detection of users' body joints and postures. Increased resolutions have now enabled a novel use of depth cameras that facilitate more fine-grained activity descriptors: The remote detection of a person's breathing by picking up the small distance changes from the user's chest over time. We propose in this work a novel method to model chest elevation to robustly monitor a user's respiration, whenever users are sitting or standing, and facing the camera. The method is robust to users occasionally blocking their torso region and is able to provide meaningful breathing features to allow classification in activity recognition tasks. We illustrate that with this method, with specific activities such as paced-breathing meditating, performing breathing exercises, or post-exercise recovery, our model delivers a breathing accuracy that matches that of a commercial respiration chest monitor belt. Results show that the breathing rate can be detected with our method at an accuracy of 92 to 97% from a distance of two metres, outperforming state-of-the-art depth imagining methods especially for non-sedentary persons, and allowing separation of activities in respiration-derived features space.
Keywords: activity recognition features; depth imaging; non-contact respiration estimation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
A novel acquisition platform for long-term breathing frequency monitoring based on inertial measurement units.Med Biol Eng Comput. 2020 Apr;58(4):785-804. doi: 10.1007/s11517-020-02125-9. Epub 2020 Jan 30. Med Biol Eng Comput. 2020. PMID: 32002753
-
Monitoring of Heart and Breathing Rates Using Dual Cameras on a Smartphone.PLoS One. 2016 Mar 10;11(3):e0151013. doi: 10.1371/journal.pone.0151013. eCollection 2016. PLoS One. 2016. PMID: 26963390 Free PMC article. Clinical Trial.
-
Breathing Analysis Using Thermal and Depth Imaging Camera Video Records.Sensors (Basel). 2017 Jun 16;17(6):1408. doi: 10.3390/s17061408. Sensors (Basel). 2017. PMID: 28621708 Free PMC article.
-
Microsoft Kinect Visual and Depth Sensors for Breathing and Heart Rate Analysis.Sensors (Basel). 2016 Jun 28;16(7):996. doi: 10.3390/s16070996. Sensors (Basel). 2016. PMID: 27367687 Free PMC article.
-
Advancements in Methods and Camera-Based Sensors for the Quantification of Respiration.Sensors (Basel). 2020 Dec 17;20(24):7252. doi: 10.3390/s20247252. Sensors (Basel). 2020. PMID: 33348827 Free PMC article. Review.
Cited by
-
Human Respiration Rate Measurement with High-Speed Digital Fringe Projection Technique.Sensors (Basel). 2023 Nov 6;23(21):9000. doi: 10.3390/s23219000. Sensors (Basel). 2023. PMID: 37960698 Free PMC article.
-
Depth-Based Measurement of Respiratory Volumes: A Review.Sensors (Basel). 2022 Dec 10;22(24):9680. doi: 10.3390/s22249680. Sensors (Basel). 2022. PMID: 36560048 Free PMC article. Review.
-
Noncontact Respiratory Monitoring Using Depth Sensing Cameras: A Review of Current Literature.Sensors (Basel). 2021 Feb 6;21(4):1135. doi: 10.3390/s21041135. Sensors (Basel). 2021. PMID: 33561970 Free PMC article. Review.
References
-
- Lara O.D., Labrador M.A. A survey on human activity recognition using wearable sensors. IEEE Commun. Surv. Tutor. 2012;15:1192–1209. doi: 10.1109/SURV.2012.110112.00192. - DOI
-
- Castro D., Coral W., Rodriguez C., Cabra J., Colorado J. Wearable-based human activity recognition using an iot approach. J. Sens. Actuator Netw. 2017;6:28. doi: 10.3390/jsan6040028. - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
