

Fast, In Vivo Model for Drug-Response Prediction in Patients with B-Cell Precursor Acute Lymphoblastic Leukemia
- PMID: 32668722
- PMCID: PMC7408814
- DOI: 10.3390/cancers12071883
Fast, In Vivo Model for Drug-Response Prediction in Patients with B-Cell Precursor Acute Lymphoblastic Leukemia
Abstract
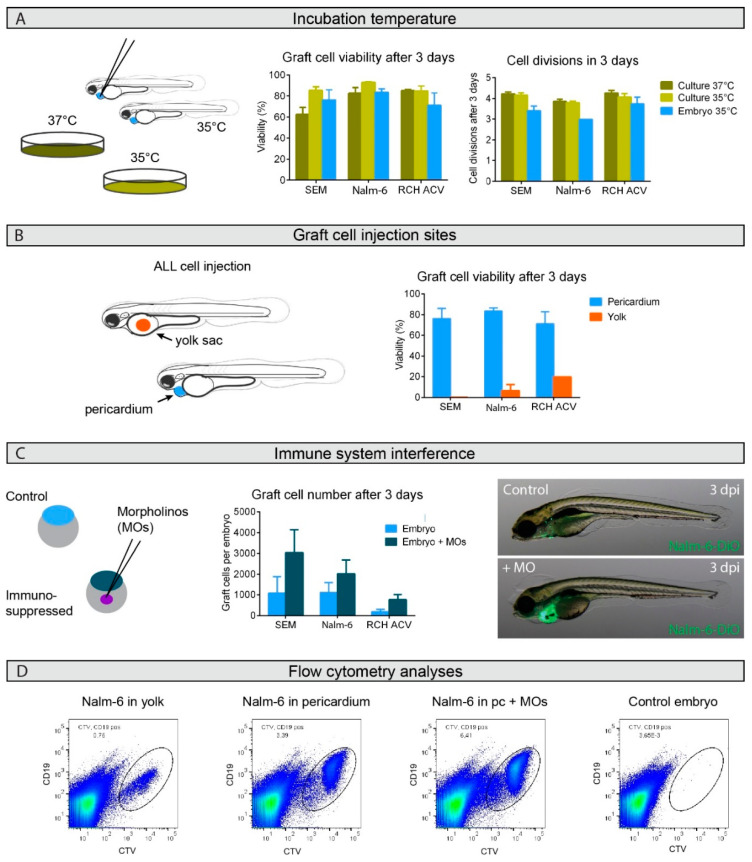
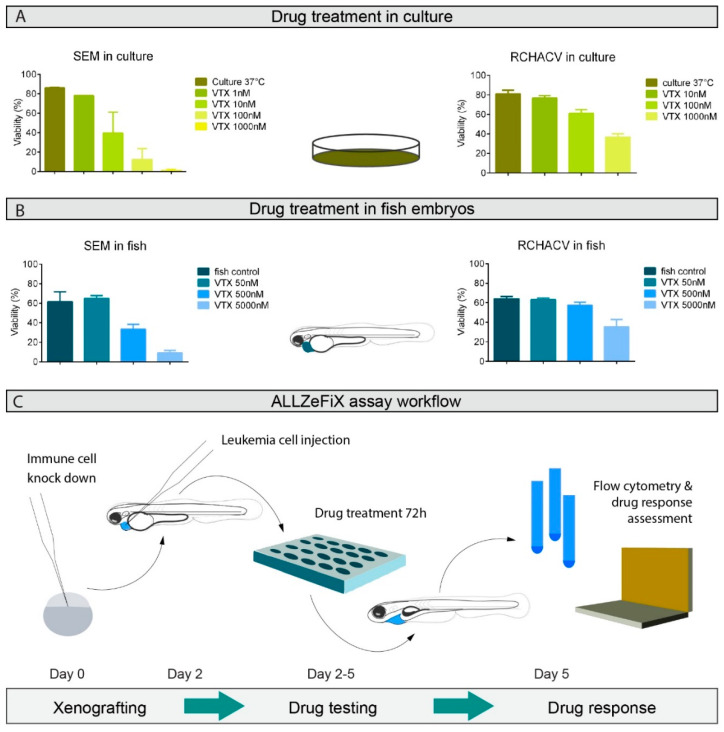
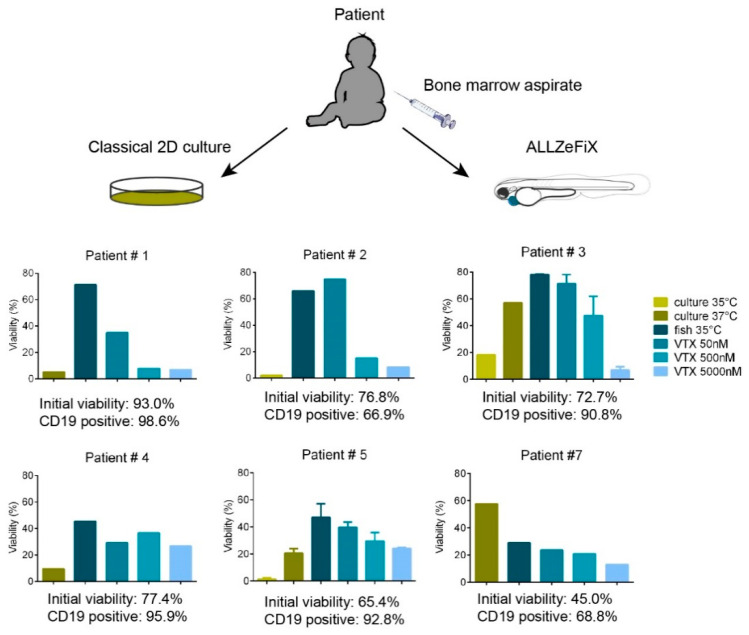
Only half of patients with relapsed B-cell precursor (BCP) acute lymphoblastic leukemia (ALL) currently survive with standard treatment protocols. Predicting individual patient responses to defined drugs prior to application would help therapy stratification and could improve survival. With the purpose to aid personalized targeted treatment approaches, we developed a human-zebrafish xenograft (ALL-ZeFiX) assay to predict drug response in a patient in 5 days. Leukemia blast cells were pericardially engrafted into transiently immunosuppressed Danio rerio embryos, and engrafted embryos treated for the test case, venetoclax, before single-cell dissolution for quantitative whole blast cell analysis. Bone marrow blasts from patients with newly diagnosed or relapsed BCP-ALL were successfully expanded in 60% of transplants in immunosuppressed zebrafish embryos. The response of BCP-ALL cell lines to venetoclax in ALL-ZeFiX assays mirrored responses in 2D cultures. Venetoclax produced varied responses in patient-derived BCP-ALL grafts, including two results mirroring treatment responses in two refractory BCP-ALL patients treated with venetoclax. Here we demonstrate proof-of-concept for our 5-day ALL-ZeFiX assay with primary patient blasts and the test case, venetoclax, which after expanded testing for further targeted drugs could support personalized treatment decisions within the clinical time window for decision-making.
Keywords: BCP-ALL; patient-derived xenograft; pediatric cancer; personalized therapy; zebrafish.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Frismantas V., Dobay M.P., Rinaldi A., Tchinda J., Dunn S.H., Kunz J., Richter-Pechanska P., Marovca B., Pail O., Jenni S., et al. Ex vivo drug response profiling detects recurrent sensitivity patterns in drug-resistant acute lymphoblastic leukemia. Blood. 2017;129:e26–e37. doi: 10.1182/blood-2016-09-738070. - DOI - PMC - PubMed
-
- Worst B.C., van Tilburg C.M., Balasubramanian G.P., Fiesel P., Witt R., Freitag A., Boudalil M., Previti C., Wolf S., Schmidt S., et al. Next-generation personalised medicine for high-risk paediatric cancer patients—The INFORM pilot study. Eur. J. Cancer. 2016;65:91–101. doi: 10.1016/j.ejca.2016.06.009. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
