

Effect of Flash Glucose Monitoring on Glycemic Control, Hypoglycemia, Diabetes-Related Distress, and Resource Utilization in the Association of British Clinical Diabetologists (ABCD) Nationwide Audit
- PMID: 32669277
- PMCID: PMC7440900
- DOI: 10.2337/dc20-0738
Effect of Flash Glucose Monitoring on Glycemic Control, Hypoglycemia, Diabetes-Related Distress, and Resource Utilization in the Association of British Clinical Diabetologists (ABCD) Nationwide Audit
Abstract
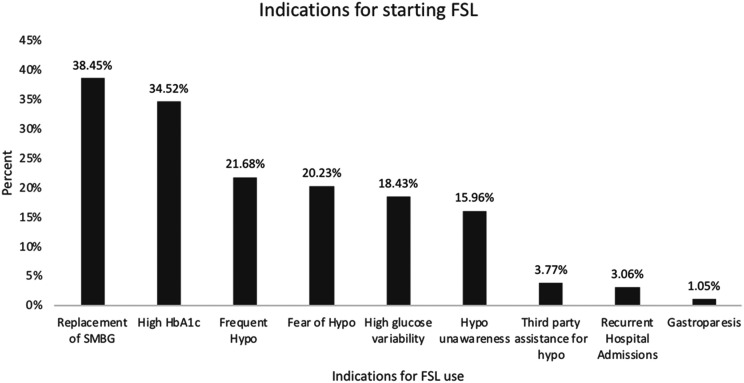
Objective: The FreeStyle Libre (FSL) flash glucose-monitoring device was made available on the U.K. National Health Service (NHS) drug tariff in 2017. This study aims to explore the U.K. real-world experience of FSL and the impact on glycemic control, hypoglycemia, diabetes-related distress, and hospital admissions.
Research design and methods: Clinicians from 102 NHS hospitals in the U.K. submitted FSL user data, collected during routine clinical care, to a secure web-based tool held within the NHS N3 network. The t and Mann-Whitney U tests were used to compare the baseline and follow-up HbA1c and other baseline demographic characteristics. Linear regression analysis was used to identify predictors of change in HbA1c following the use of FSL. Within-person variations of HbA1c were calculated using [Formula: see text].
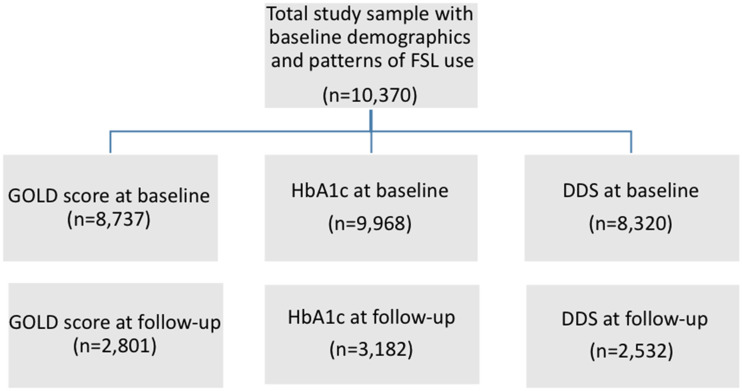
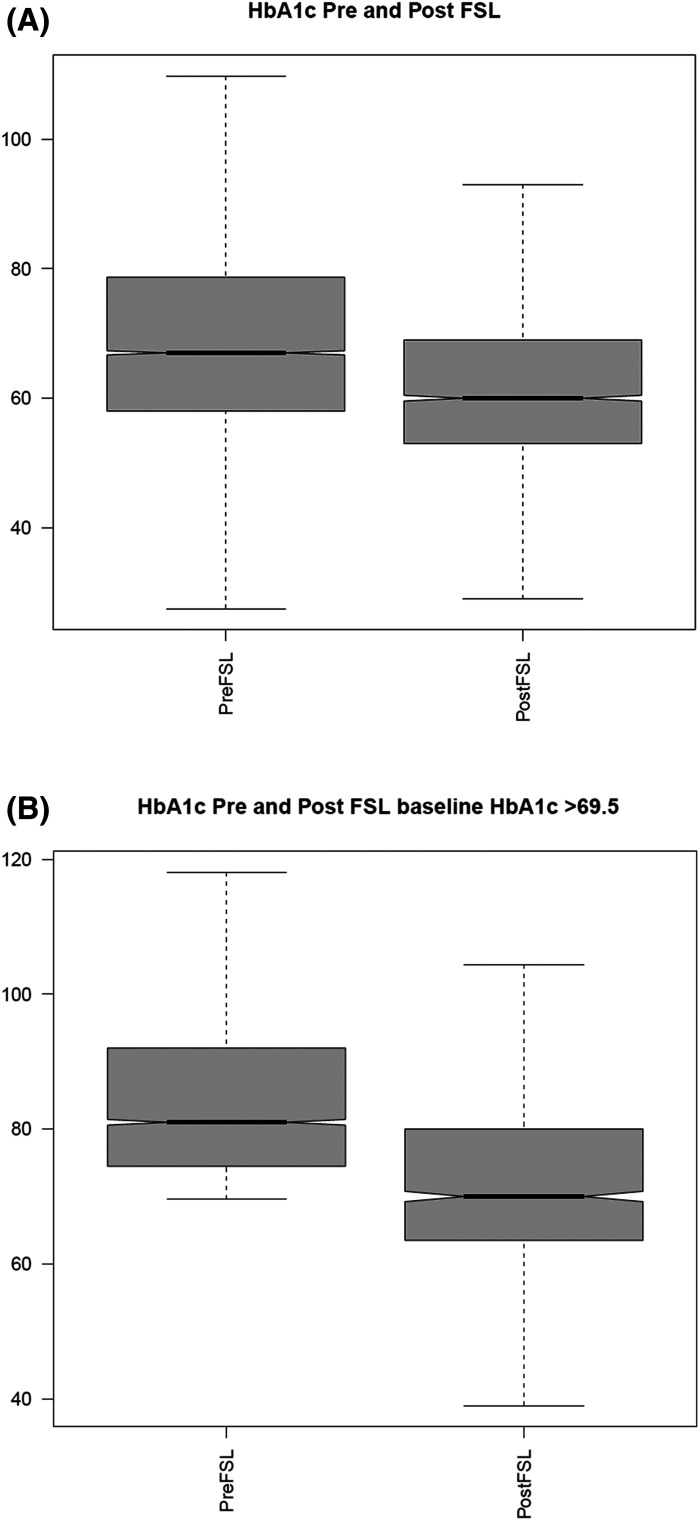
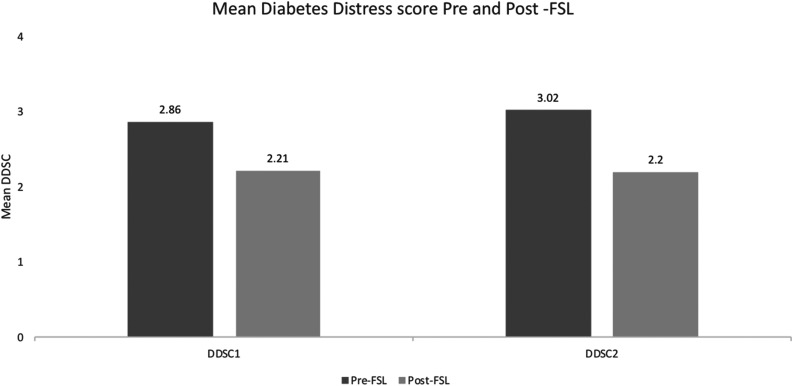
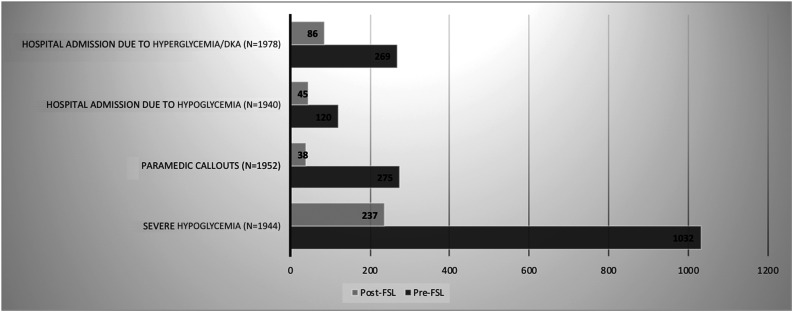
Results: Data were available for 10,370 FSL users (97% with type 1 diabetes), age 38.0 (±18.8) years, 51% female, diabetes duration 16.0 (±49.9) years, and BMI of 25.2 (±16.5) kg/m2 (mean [±SD]). FSL users demonstrated a -5.2 mmol/mol change in HbA1c, reducing from 67.5 (±20.9) mmol/mol (8.3%) at baseline to 62.3 (±18.5) mmol/mol (7.8%) after 7.5 (interquartile range 3.4-7.8) months of follow-up (n = 3,182) (P < 0.0001). HbA1c reduction was greater in those with initial HbA1c ≥69.5 mmol/mol (>8.5%), reducing from 85.5 (±16.1) mmol/mol (10%) to 73.1 (±15.8) mmol/mol (8.8%) (P < 0.0001). The baseline Gold score (score for hypoglycemic unawareness) was 2.7 (±1.8) and reduced to 2.4 (±1.7) (P < 0.0001) at follow-up. A total of 53% of those with a Gold score of ≥4 at baseline had a score <4 at follow-up. FSL use was also associated with a reduction in diabetes distress (P < 0.0001). FSL use was associated with a significant reduction in paramedic callouts and hospital admissions due to hypoglycemia and hyperglycemia/diabetic ketoacidosis.
Conclusions: We show that the use of FSL was associated with significantly improved glycemic control and hypoglycemia awareness and a reduction in hospital admissions.
© 2020 by the American Diabetes Association.
Figures
References
-
- Beck RW, Riddlesworth T, Ruedy K, et al. .; DIAMOND Study Group . Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections: the DIAMOND Randomized Clinical Trial. JAMA 2017;317:371–378 - PubMed
-
- Heinemann L, Deiss D, Hermanns N, et al. . HypoDE: research design and methods of a randomized controlled study evaluating the impact of real-time CGM usage on the frequency of CGM glucose values <55 mg/dl in patients with type 1 diabetes and problematic hypoglycemia treated with multiple daily injections. J Diabetes Sci Technol 2015;9:651–662 - PMC - PubMed
-
- Heinemann L, Freckmann G, Ehrmann D, et al. . Real-time continuous glucose monitoring in adults with type 1 diabetes and impaired hypoglycaemia awareness or severe hypoglycaemia treated with multiple daily insulin injections (HypoDE): a multicentre, randomised controlled trial. Lancet 2018;391:1367–1377 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
