

Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis
- PMID: 32669282
- PMCID: PMC7362233
- DOI: 10.1136/bmj.m2297
Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis
Abstract
Objective: To evaluate the associations between prediabetes and the risk of all cause mortality and incident cardiovascular disease in the general population and in patients with a history of atherosclerotic cardiovascular disease.
Design: Updated meta-analysis.
Data sources: Electronic databases (PubMed, Embase, and Google Scholar) up to 25 April 2020.
Review methods: Prospective cohort studies or post hoc analysis of clinical trials were included for analysis if they reported adjusted relative risks, odds ratios, or hazard ratios of all cause mortality or cardiovascular disease for prediabetes compared with normoglycaemia. Data were extracted independently by two investigators. Random effects models were used to calculate the relative risks and 95% confidence intervals. The primary outcomes were all cause mortality and composite cardiovascular disease. The secondary outcomes were the risk of coronary heart disease and stroke.
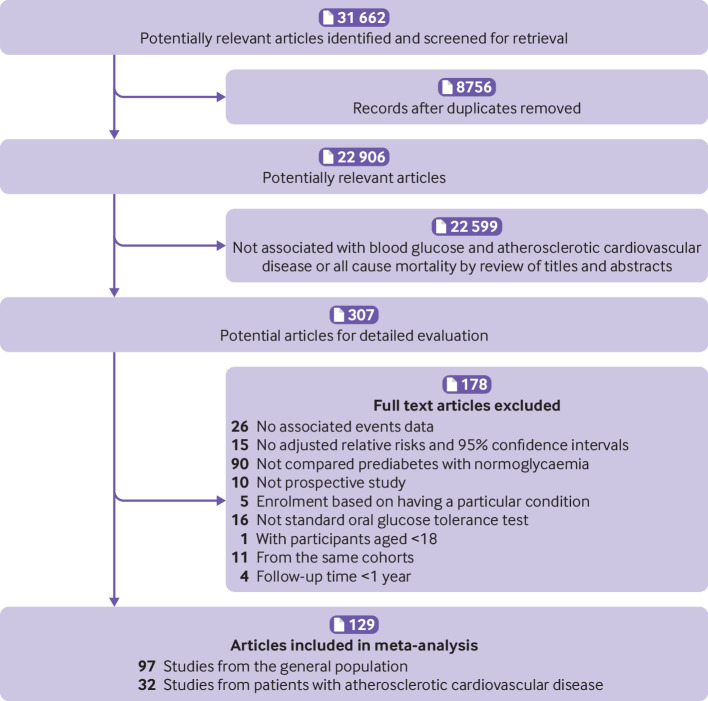
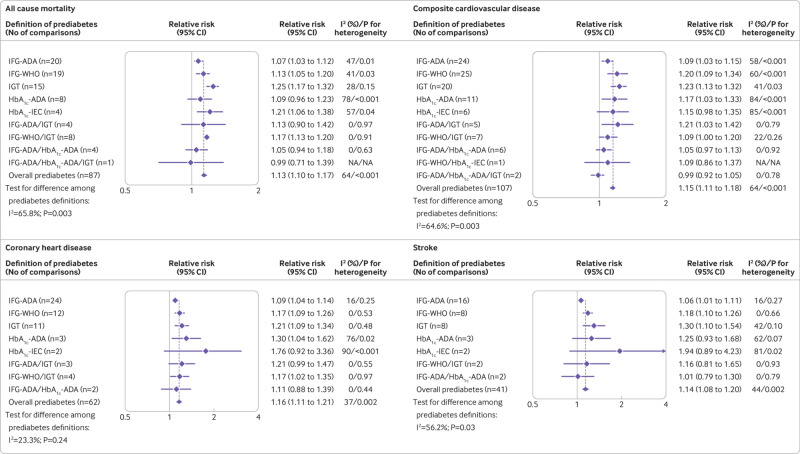
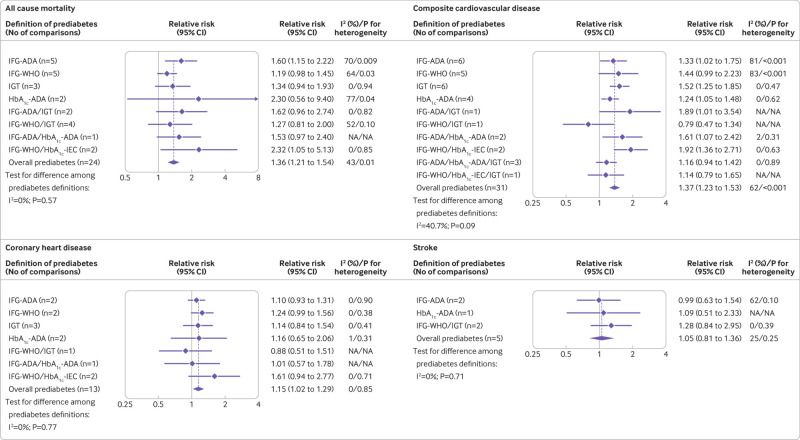
Results: A total of 129 studies were included, involving 10 069 955 individuals for analysis. In the general population, prediabetes was associated with an increased risk of all cause mortality (relative risk 1.13, 95% confidence interval 1.10 to 1.17), composite cardiovascular disease (1.15, 1.11 to 1.18), coronary heart disease (1.16, 1.11 to 1.21), and stroke (1.14, 1.08 to 1.20) in a median follow-up time of 9.8 years. Compared with normoglycaemia, the absolute risk difference in prediabetes for all cause mortality, composite cardiovascular disease, coronary heart disease, and stroke was 7.36 (95% confidence interval 9.59 to 12.51), 8.75 (6.41 to 10.49), 6.59 (4.53 to 8.65), and 3.68 (2.10 to 5.26) per 10 000 person years, respectively. Impaired glucose tolerance carried a higher risk of all cause mortality, coronary heart disease, and stroke than impaired fasting glucose. In patients with atherosclerotic cardiovascular disease, prediabetes was associated with an increased risk of all cause mortality (relative risk 1.36, 95% confidence interval 1.21 to 1.54), composite cardiovascular disease (1.37, 1.23 to 1.53), and coronary heart disease (1.15, 1.02 to 1.29) in a median follow-up time of 3.2 years, but no difference was seen for the risk of stroke (1.05, 0.81 to 1.36). Compared with normoglycaemia, in patients with atherosclerotic cardiovascular disease, the absolute risk difference in prediabetes for all cause mortality, composite cardiovascular disease, coronary heart disease, and stroke was 66.19 (95% confidence interval 38.60 to 99.25), 189.77 (117.97 to 271.84), 40.62 (5.42 to 78.53), and 8.54 (32.43 to 61.45) per 10 000 person years, respectively. No significant heterogeneity was found for the risk of all outcomes seen for the different definitions of prediabetes in patients with atherosclerotic cardiovascular disease (all P>0.10).
Conclusions: Results indicated that prediabetes was associated with an increased risk of all cause mortality and cardiovascular disease in the general population and in patients with atherosclerotic cardiovascular disease. Screening and appropriate management of prediabetes might contribute to primary and secondary prevention of cardiovascular disease.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: support from the Guangdong Basic and Applied Basic Research Fund, Science and Technology Innovation Project, and Clinical Research Startup Programme of Shunde Hospital, Southern Medical University for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous