

Primary Care Provider Beliefs and Recommendations About Colorectal Cancer Screening in Four Healthcare Systems
- PMID: 32669318
- PMCID: PMC7641998
- DOI: 10.1158/1940-6207.CAPR-20-0109
Primary Care Provider Beliefs and Recommendations About Colorectal Cancer Screening in Four Healthcare Systems
Abstract
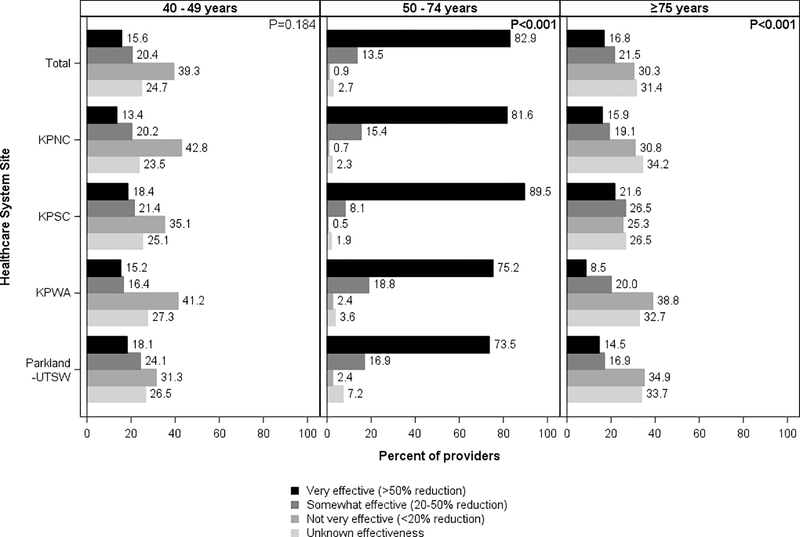
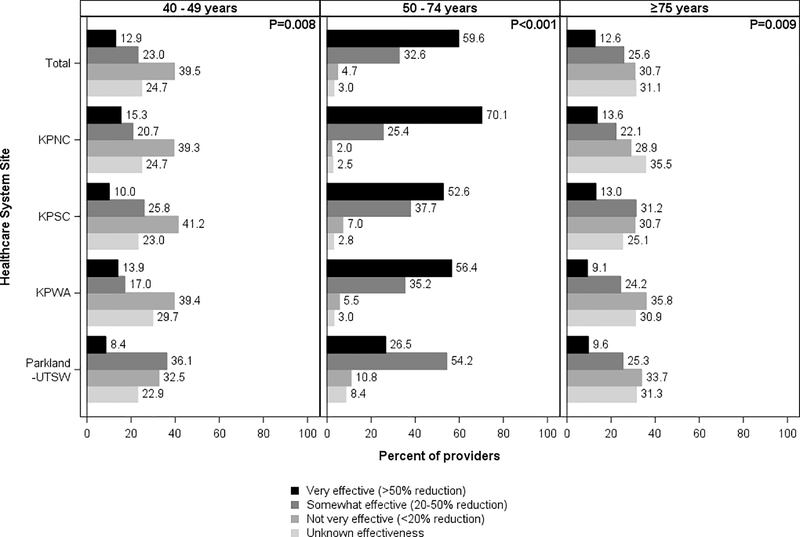
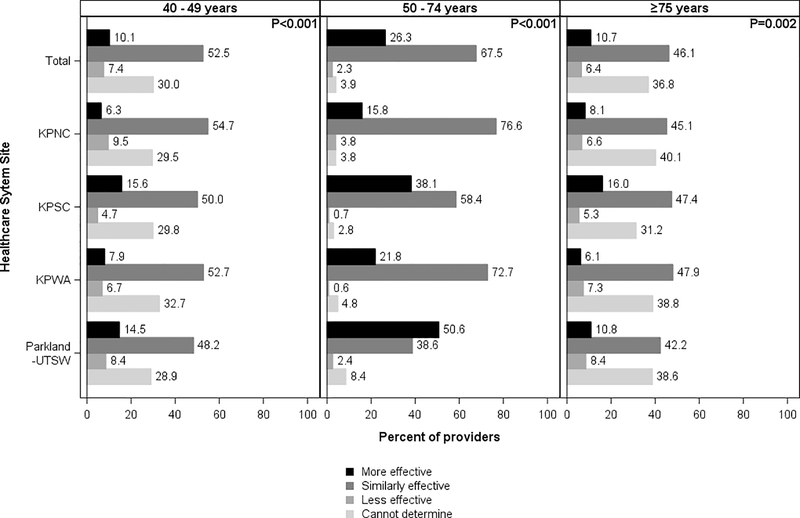
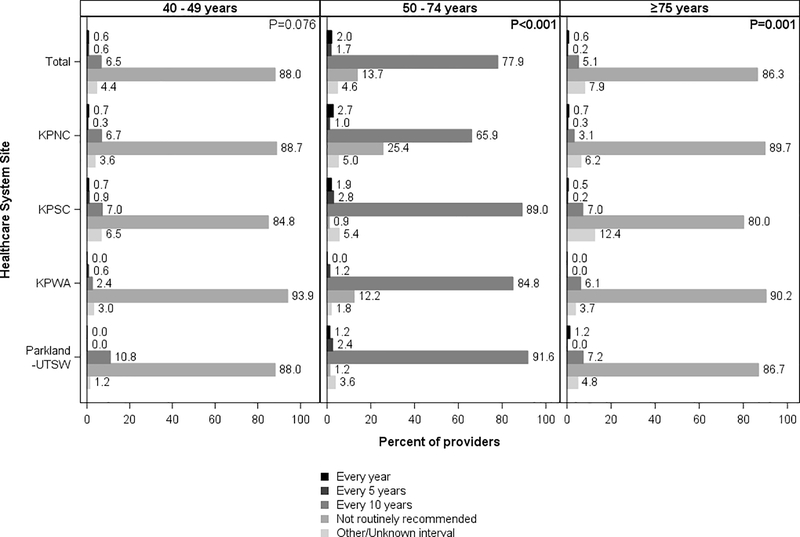
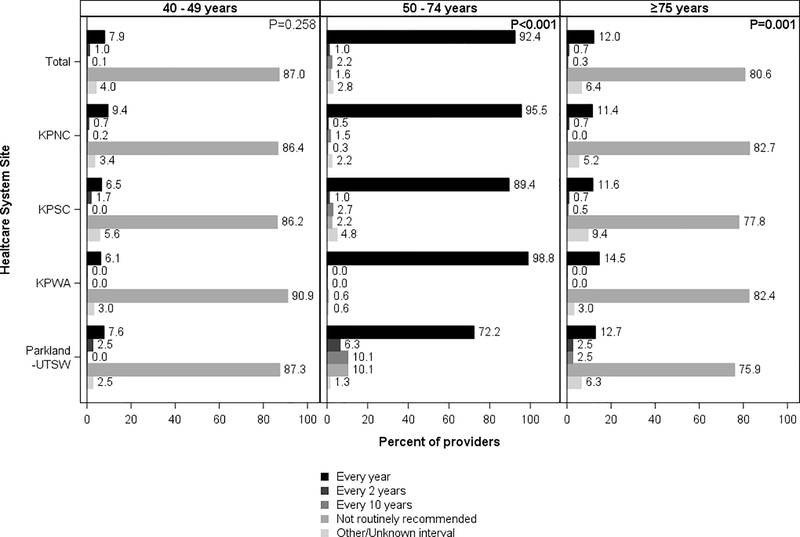
Primary care provider's (PCP) perceptions of colorectal cancer screening test effectiveness and their recommendations for testing intervals influence patient screening uptake. Few large studies have examined providers' perceptions and recommendations, including their alignment with evidence suggesting comparable test effectiveness and guideline recommendations for screening frequency. Providers (n = 1,281) within four healthcare systems completed a survey in 2017-2018 regarding their perceptions of test effectiveness and recommended intervals for colonoscopy and fecal immunochemical testing (FIT) for patients ages 40-49, 50-74, and ≥75 years. For patients 50-74 (screening eligible), 82.9% of providers rated colonoscopy as very effective versus 59.6% for FIT, and 26.3% rated colonoscopy as more effective than FIT. Also, for this age group, 77.9% recommended colonoscopy every 10 years and 92.4% recommended FIT annually. For patients ages 40-49 and ≥75, more than one-third of providers believed the tests were somewhat or very effective, although >80% did not routinely recommend screening by either test for these age groups. Provider screening test interval recommendations generally aligned with colorectal cancer guidelines; however, 25% of providers believed colonoscopy was more effective than FIT for mortality reduction, which differs from some modeling studies that suggest comparable effectiveness. The latter finding may have implications for health systems where FIT is the dominant screening strategy. Only one-third of providers reported believing these screening tests were effective in younger and older patients (i.e., <50 and ≥75 years). Evidence addressing these beliefs may be relevant if cancer screening recommendations are modified to include older and/or younger patients.
©2020 American Association for Cancer Research.
Conflict of interest statement
Conflict of Interest
The authors declare no potential conflicts of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019;69:7–34. - PubMed
-
- Brenner H, Chang-Claude J, Seiler CM, et al. Protection from colorectal cancer after colonoscopy: a population-based, case-control study. Ann Intern Med 2011;154:22–30. - PubMed
-
- About 80% by 2018: National Colorectal Cancer Roundtable.
-
- Benson VS, Atkin WS, Green J, et al. Toward standardizing and reporting colorectal cancer screening indicators on an international level: The International Colorectal Cancer Screening Network. Int J Cancer 2012;130:2961–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
