

Clinical Characteristics and Immune Injury Mechanisms in 71 Patients with COVID-19
- PMID: 32669467
- PMCID: PMC7364211
- DOI: 10.1128/mSphere.00362-20
Clinical Characteristics and Immune Injury Mechanisms in 71 Patients with COVID-19
Abstract
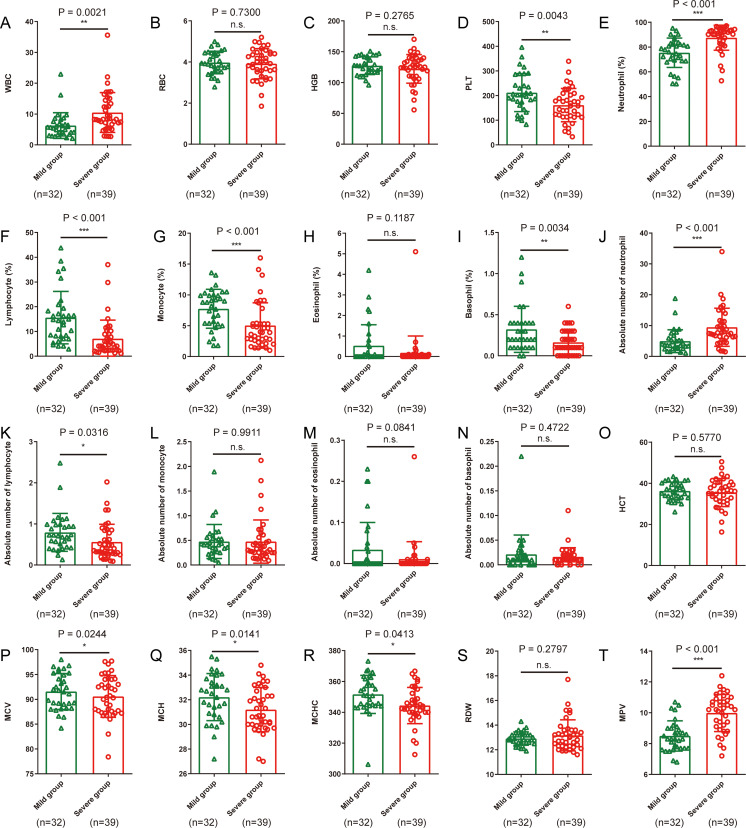
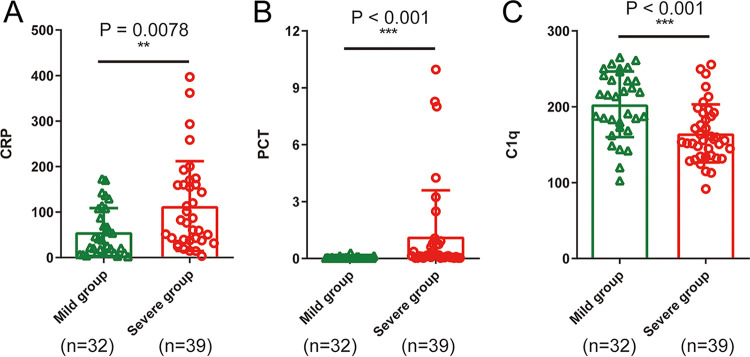
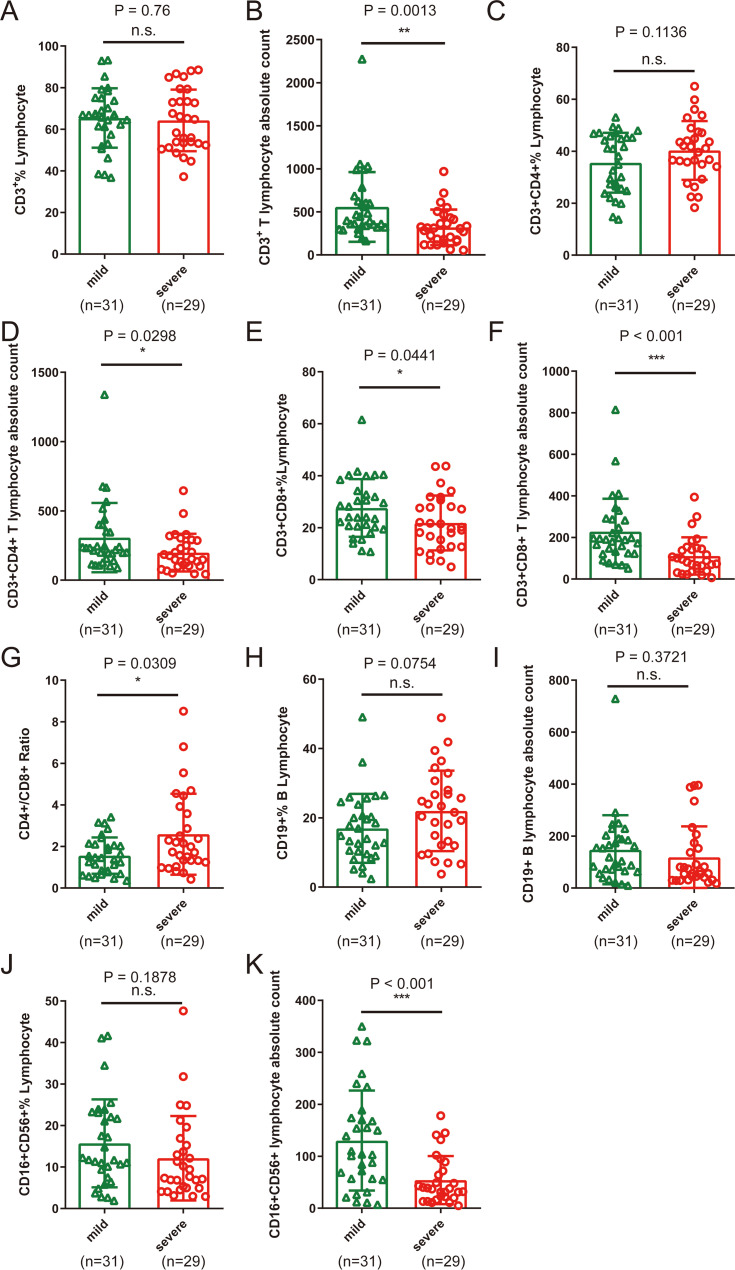
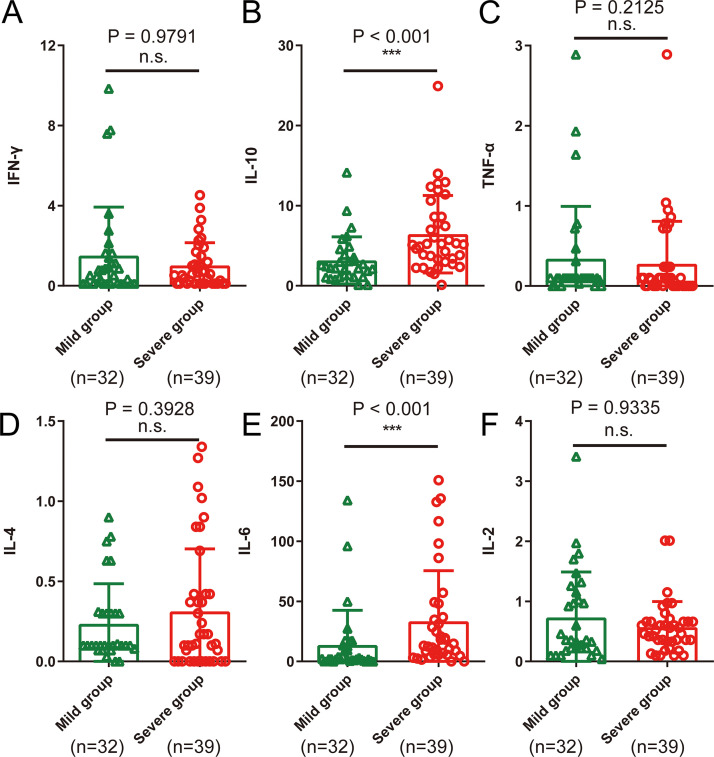
The outbreak of coronavirus disease 2019 (COVID-19), caused by the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has caused a threat to global health. The mortality rate of severely ill patients in the early stage is 32.5%. The exacerbation of the condition and death of patients are closely associated with inflammatory cytokine storms, which are caused by excessive activation of the immune and complement systems as well as the coinfection of other pathogens. However, the immunological characteristics and the mechanisms underlying inflammatory storms have not been well elucidated. Here, we analyzed the clinical and immunological characteristics of 71 confirmed COVID-19 patients. Based on the National Health Commission of China (NHCC) guidelines, patients were stratified into mild and severe types. We compared the clinical and laboratory data obtained from electronic medical records between the two types. In regard to the hematological parameters, COVID-19 patients showed decreased erythrocyte count, hemoglobin, hematocrit, lymphocyte count, eosinophil count, and complement C1q, whereas neutrophils, C-reactive protein, and procalcitonin were significantly increased, especially in severe cases. We also found that CD3+ CD4+ T lymphocytes, CD3+ CD8+ T lymphocytes, CD19+ B lymphocytes, and CD16+ CD56+ NK cells in the peripheral blood of all patients were decreased. In addition, CD3+ CD8+ T lymphocytes, CD16+ CD56+ NK cells, and complement C1q in severely ill patients decreased more significantly. Additionally, interleukin 6 (IL-6) elevation was particularly prominent in all patients, especially in severe cases. These results suggest that CD3+ CD8+ T lymphocytes, CD16+ CD56+ NK cells, C1q as well as IL-6 may play critical roles in the inflammatory cytokine storm. The dysregulation of these aforementioned immune parameters, along with bacterial coinfection, were the important causes of exacerbation of the patients' condition and death. This study improves our understanding of the immune dysregulation of COVID-19 and provides potential immunotherapeutic strategies.IMPORTANCE The dysregulation of CD3+ CD8+ T lymphocytes, CD16+ CD56+ NK cells, C1q as well as IL-6, along with bacterial coinfection, were important causes of exacerbation of the patients' condition and death.
Keywords: COVID-19; SARS-CoV-2; coronavirus; immunological characteristics; infection; inflammatory cytokine storm.
Copyright © 2020 Wu et al.
Figures
References
-
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L. 2020. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395:507–513. doi: 10.1016/S0140-6736(20)30211-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
