

Epidemiology of Neuromyelitis Optica Spectrum Disorder and Its Prevalence and Incidence Worldwide
- PMID: 32670177
- PMCID: PMC7332882
- DOI: 10.3389/fneur.2020.00501
Epidemiology of Neuromyelitis Optica Spectrum Disorder and Its Prevalence and Incidence Worldwide
Abstract
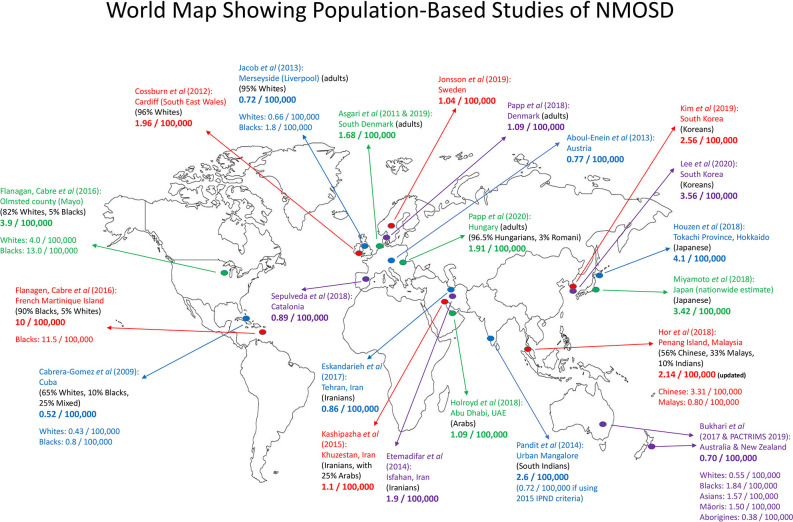
Neuromyelitis optica spectrum disorder (NMOSD) is an uncommon inflammatory disease of the central nervous system, manifesting clinically as optic neuritis, myelitis, and certain brain and brainstem syndromes. Cases clinically diagnosed as NMOSD may include aquaporin 4 (AQP4)-antibody-seropositive autoimmune astrocytopathic disease, myelin oligodendrocyte glycoprotein (MOG)-antibody-seropositive inflammatory demyelinating disease, and double-seronegative disease. AQP4-antibody disease has a high female-to-male ratio (up to 9:1), and its mean age at onset of ~40 years is later than that seen in multiple sclerosis. For MOG-antibody disease, its gender ratio is closer to 1:1, and it is more common in children than in adults. Its clinical phenotypes differ but overlap with those of AQP4-antibody disease and include acute disseminated encephalomyelitis, brainstem and cerebral cortical encephalitis, as well as optic neuritis and myelitis. Double-seronegative disease requires further research and clarification. Population-based studies over the past two decades report the prevalence and incidence of NMOSD in different populations worldwide. One relevant finding is the varying prevalence observed in different racial groups. Consistently, the prevalence of NMOSD among Whites is ~1/100,000 population, with an annual incidence of <1/million population. Among East Asians, the prevalence is higher, at ~3.5/100,000 population, while the prevalence in Blacks may be up to 10/100,000 population. For MOG-antibody disease, hospital-based studies largely do not observe any significant racial preponderance so far. This disorder comprises a significant proportion of NMOSD cases that are AQP4-antibody-seronegative. A recent Dutch nationwide study reported the annual incidence of MOG-antibody disease as 1.6/million population (adult: 1.3/million, children: 3.1/million). Clinical and radiological differences between AQP4-antibody and MOG-antibody associated diseases have led to interest in the revisions of NMOSD definition and expanded stratification based on detection of a specific autoantibody biomarker. More population-based studies in different geographical regions and racial groups will be useful to further inform the prevalence and incidence of NMOSD and their antibody-specific subgroups. Accessibility to AQP4-antibody and MOG-antibody testing, which is limited in many centers, is a challenge to overcome. Environmental and genetic studies will be useful accompaniments to identify other potential pathogenetic factors and specific biomarkers in NMOSD.
Keywords: AQP4; MOG; NMOSD; epidemiology; incidence; neuromyelitis optica spectrum disorder; population study; prevalence.
Copyright © 2020 Hor, Asgari, Nakashima, Broadley, Leite, Kissani, Jacob, Marignier, Weinshenker, Paul, Pittock, Palace, Wingerchuk, Behne, Yeaman and Fujihara.
Figures
References
-
- Fujihara K, Misu T, Nakashima I, Takahashi T, Bradl M, Lassmann H, et al. Neuromyelitis optica should be classified as an astrocytopathic disease rather than a demyelinating disease. Clin Exp Neuroimmunol. (2012) 3:58–73. 10.1111/j.1759-1961.2012.00030.x - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous