

Is Office Laryngoscopy an Aerosol-Generating Procedure?
- PMID: 32671840
- PMCID: PMC7404375
- DOI: 10.1002/lary.28973
Is Office Laryngoscopy an Aerosol-Generating Procedure?
Abstract
Objectives/hypothesis: The aims of this work were 1) to investigate whether office laryngoscopy is an aerosol-generating procedure with an optical particle sizer (OPS) during clinical simulation on healthy volunteers, and 2) to critically discuss methods for assessment of aerosolizing potentials in invasive interventions.
Study design: Prospective quantification of aerosol and droplet generation during clinical simulation of rigid and flexible laryngoscopy.
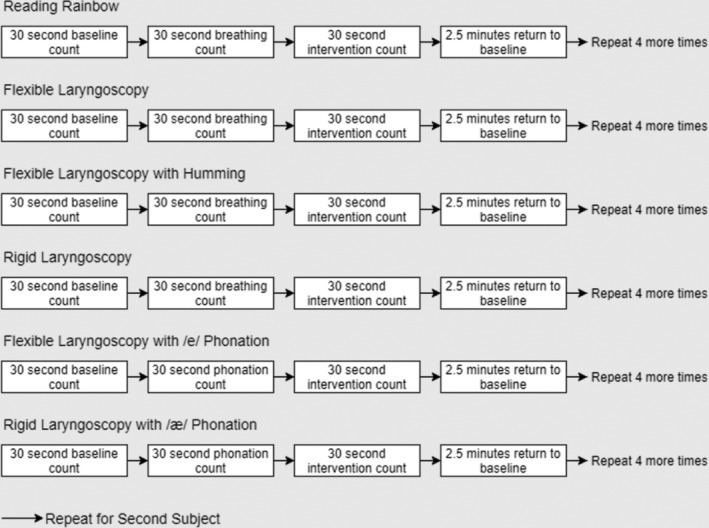
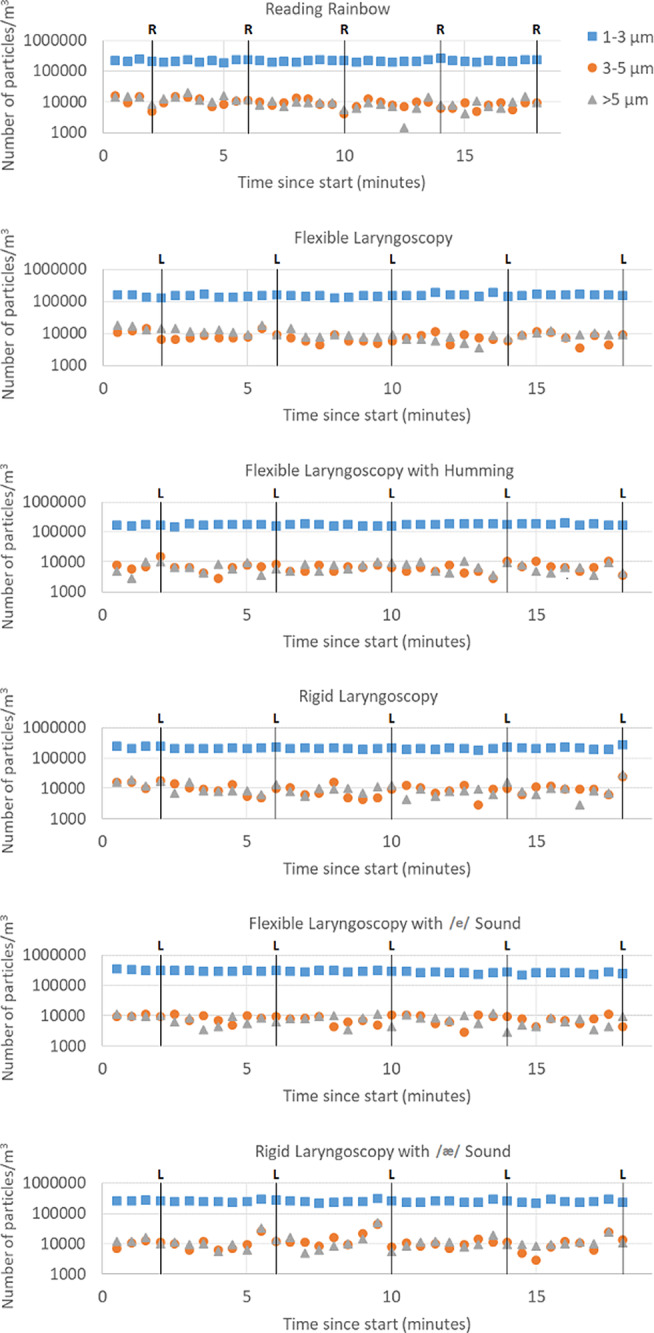
Methods: Two healthy volunteers were recruited to undergo both flexible and rigid laryngoscopy. An OPS was used to quantify aerosols and droplets generated for four positive controls relative to ambient particles (speech, breathing, /e/ phonation, and /ae/ phonation) and for five test interventions relative to breathing and phonation (flexible laryngoscopy, flexible laryngoscopy with humming, flexible laryngoscopy with /e/ phonation, rigid laryngoscopy, and rigid laryngoscopy with /ae/ phonation). Particle counts in mean diameter size range from 0.3 to >10 μm were measured with OPS placed at 12 cm from the subject's nose/mouth.
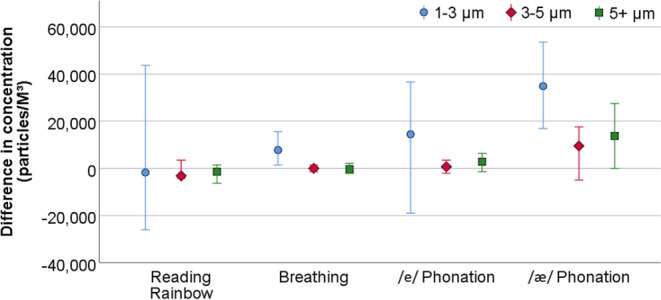
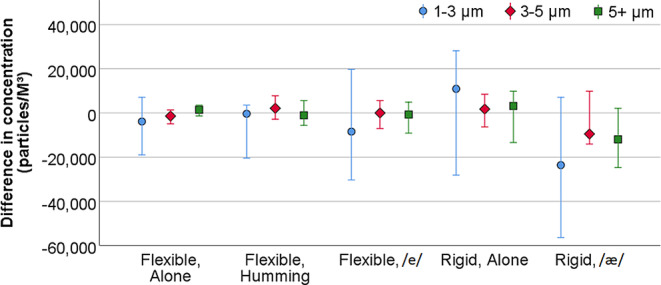
Results: None of the laryngoscopy interventions (n = 10 each) generated aerosols above that produced by breathing or phonation. Breathing (n = 40, 1-3 μm, P = .016) and /ae/ phonation (n = 10, 1-3 μm, P = .022; 3-5 μm. P = .083; >5 μm, P = .012) were statistically significant producers of aerosols and droplets. Neither speech nor /e/ phonation (n = 10 each) were associated with statistically significant aerosols and droplet generation.
Conclusions: Using OPS to detect droplets and aerosols, we found that office laryngoscopy is likely not an aerosol-generating procedure. Despite its prior use in otolaryngological literature, an OPS has intrinsic limitations. Our study should be complemented with more sophisticated methods of droplet distribution measurement.
Level of evidence: 3 Laryngoscope, 130:2637-2642, 2020.
Keywords: Flexible laryngoscopy; aerosol-generating procedures; droplet quantification; optical particle sizer; rigid laryngoscopy.
© 2020 American Laryngological, Rhinological and Otological Society Inc, The Triological Society and American Laryngological Association (ALA).
Figures

References
-
- Micik RE, Miller RL, Mazzarella MA, Ryge G. Studies on dental aerobiology: I. bacterial aerosols generated during dental procedures. J Dent Res 1969;48:49–56. - PubMed
-
- Bentley CD, Burkhart NW, Crawford JJ. Evaluating spatter and aerosol contamination during dental procedures. J Am Dent Assoc 1994;125:579–584. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
