

National Trends in the Prevalence of Chronic Kidney Disease Among Racial/Ethnic and Socioeconomic Status Groups, 1988-2016
- PMID: 32672828
- PMCID: PMC7366187
- DOI: 10.1001/jamanetworkopen.2020.7932
National Trends in the Prevalence of Chronic Kidney Disease Among Racial/Ethnic and Socioeconomic Status Groups, 1988-2016
Erratum in
-
Error in Figure.JAMA Netw Open. 2020 Aug 3;3(8):e2019157. doi: 10.1001/jamanetworkopen.2020.19157. JAMA Netw Open. 2020. PMID: 32804208 Free PMC article. No abstract available.
Abstract
Importance: The overall prevalence of chronic kidney disease (CKD) has stabilized in the United States in recent years. However, it is unclear whether all major sociodemographic groups experienced this trend.
Objective: To examine trends in CKD prevalence across major sociodemographic groups as defined by race/ethnicity and socioeconomic status.
Design, setting, and participants: This repeated cross-sectional study used data from the National Health and Nutrition Examination Surveys for 1988 to 1994 and every 2 years from 1999 to 2016 on individuals 20 years or older with information on race/ethnicity, socioeconomic status, and serum creatinine levels. Statistical analysis was conducted from May 1, 2017, to April 6, 2020.
Exposures: Race/ethnicity and socioeconomic status.
Main outcomes and measures: Prevalence of CKD was defined as an estimated glomerular filtration rate of 15 to 59 mL/min/1.73 m2.
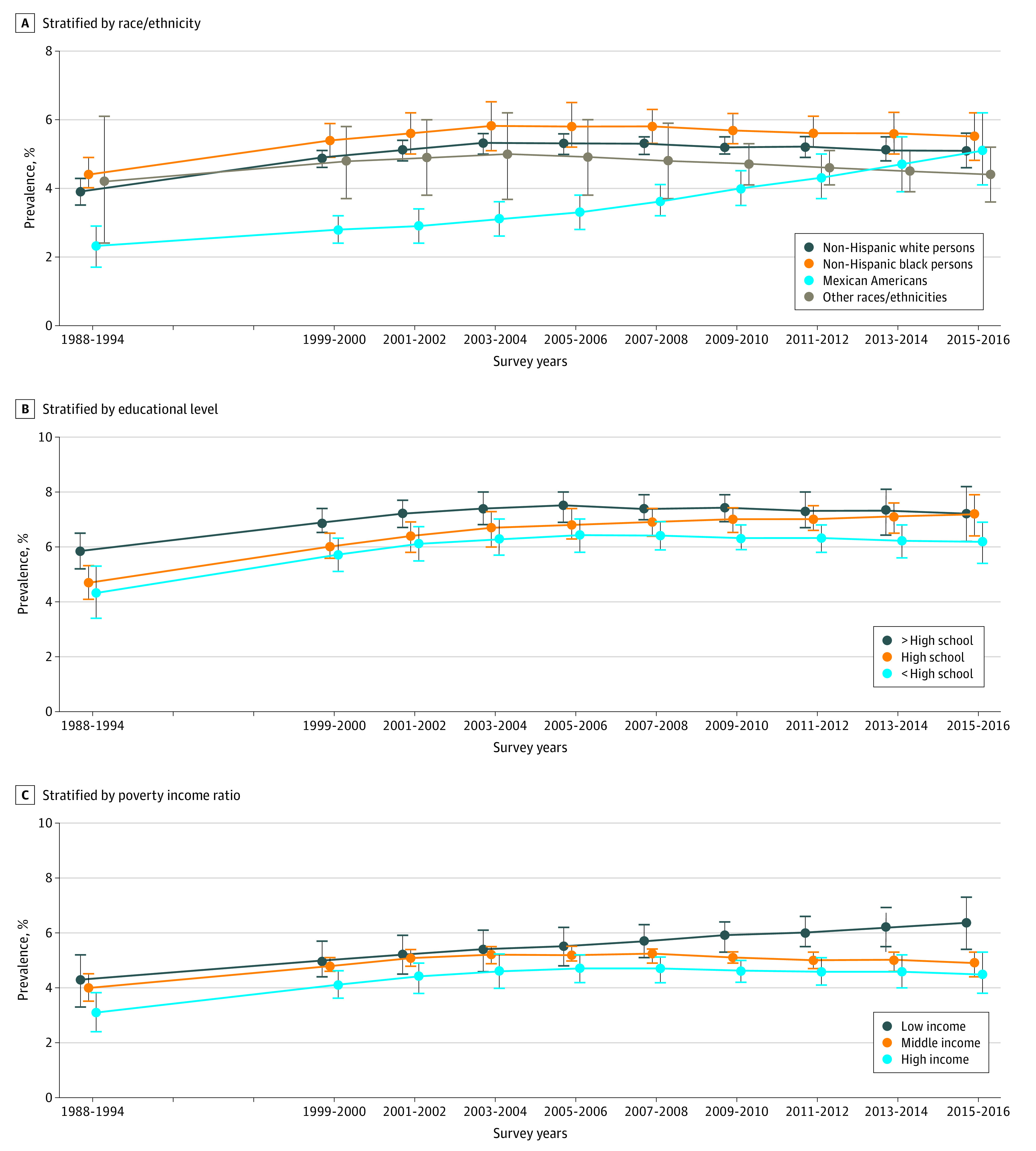
Results: A total of 54 554 participants (mean [SE] age, 46.2 [0.2] years; 51.7% female) were examined. The age-, sex- and race/ethnicity-adjusted overall prevalence of stage 3 and 4 CKD increased from 3.9% in 1988-1994 to 5.2% in 2003-2004 (difference, 1.3%; 95% CI, 0.9%-1.7%; P < .001 for change) and remained relatively stable thereafter at 5.1% in 2015-2016 (difference, -0.1%; 95% CI, -0.7% to 0.4%; P = .61 for change). The trend in adjusted CKD prevalence differed significantly by race/ethnicity (P = .009 for interaction). In non-Hispanic white and non-Hispanic black persons, CKD prevalence increased between 1988-1994 and 2003-2004 and remained stable thereafter. Among Mexican American persons, CKD prevalence was lower than in other racial/ethnic groups and remained stable between 1988-1994 and 2003-2004 but nearly doubled (difference, 2.1%; 95% CI, 0.9%-3.3%; P = .001 for change) between 2003-2004 and 2015-2016 to rates similar to those in other racial/ethnic groups. There were higher rates of CKD prevalence among groups with lower educational level and income (eg, 5.8% vs 4.3% and 4.3% vs 3.1% in low vs high education and income, respectively, in 1988-1994), but trends in CKD prevalence mirrored those for the overall population. The higher CKD prevalence among individuals with lower educational level and income remained largely consistent throughout the entire period. Results were similar in most subgroups when including albuminuria to define CKD.
Conclusions and relevance: The prevalence of CKD in the United States has stabilized overall in recent years but has increased among Mexican American persons. More important, gaps in CKD prevalence across racial/ethnic groups and levels of socioeconomic status largely persisted over 28 years. There is a need to identify and address causes of increasing CKD prevalence among Mexican American persons and a need to renew efforts to effectively mitigate persistent disparities in CKD prevalence.
Conflict of interest statement
Figures
References
-
- Astor BC, Matsushita K, Gansevoort RT, et al. ; Chronic Kidney Disease Prognosis Consortium . Lower estimated glomerular filtration rate and higher albuminuria are associated with mortality and end-stage renal disease: a collaborative meta-analysis of kidney disease population cohorts. Kidney Int. 2011;79(12):1331-1340. doi: 10.1038/ki.2010.550 - DOI - PMC - PubMed
-
- Gansevoort RT, Matsushita K, van der Velde M, et al. ; Chronic Kidney Disease Prognosis Consortium . Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes: a collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80(1):93-104. doi: 10.1038/ki.2010.531 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
