

Effect of Cold Atmospheric Plasma Therapy vs Standard Therapy Placebo on Wound Healing in Patients With Diabetic Foot Ulcers: A Randomized Clinical Trial
- PMID: 32672829
- PMCID: PMC7366186
- DOI: 10.1001/jamanetworkopen.2020.10411
Effect of Cold Atmospheric Plasma Therapy vs Standard Therapy Placebo on Wound Healing in Patients With Diabetic Foot Ulcers: A Randomized Clinical Trial
Erratum in
-
Numeric Errors in Figure 3.JAMA Netw Open. 2020 Oct 1;3(10):e2024427. doi: 10.1001/jamanetworkopen.2020.24427. JAMA Netw Open. 2020. PMID: 33006615 Free PMC article. No abstract available.
Abstract
Importance: Diabetic foot ulcers are a common complication of diabetes and require specialized treatment. Cold atmospheric plasma (CAP) has been associated with benefits in wound infection and healing in previous smaller series of case reports. Yet the effect of CAP compared with standard care therapy in wound healing in diabetic foot ulcers remains to be studied.
Objective: To determine whether the application of CAP accelerates wound healing in diabetic foot ulcers compared with standard care therapy.
Design, setting, and participants: A prospective, randomized, placebo-controlled, patient-blinded clinical trial was conducted at 2 clinics with recruitment from August 17, 2016, to April 20, 2019. Patients were scheduled to remain in follow-up until April 30, 2024. Patients with diabetes and diabetic foot ulcers described using the combined Wagner-Armstrong classification of 1B or 2B (superficial or infected diabetic foot ulcers extending to tendon) were eligible. A patient could participate with 1 or more wounds in both groups in both intervention and control groups. Wounds were randomized separately, allowing a participant to be treated several times within the study following a 2 × 2 × 2 randomization strata considering sex, smoking status, and age (≤68 years and >68 years).
Interventions: Standard care treatment with 8 applications of either CAP generated from argon gas in an atmospheric pressure plasma jet or 8 applications of placebo treatment in a patient-blinded manner.
Main outcomes and measures: Primary end points were reduction in wound size, clinical infection, and microbial load compared with treatment start. Secondary end points were time to relevant wound reduction (>10%), reduction of infection, parameters of patient's well-being, and treatment-associated adverse events.
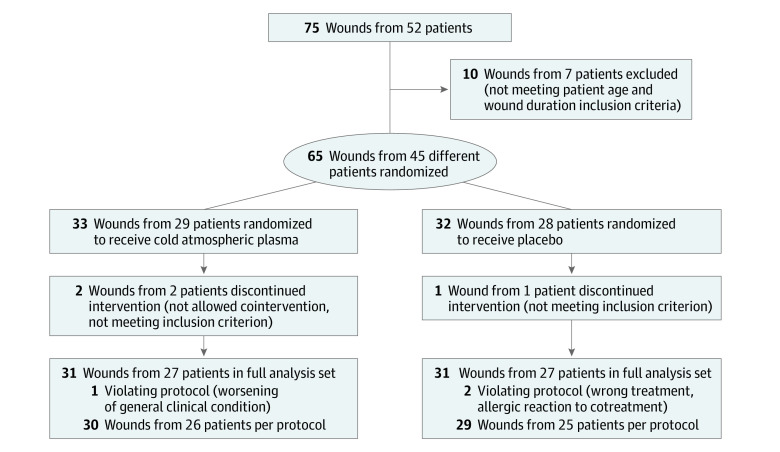
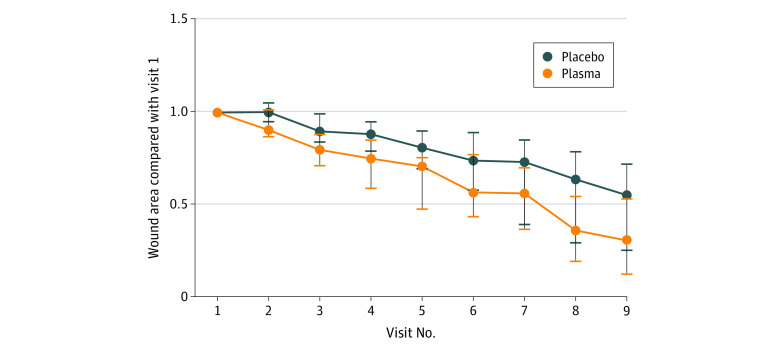
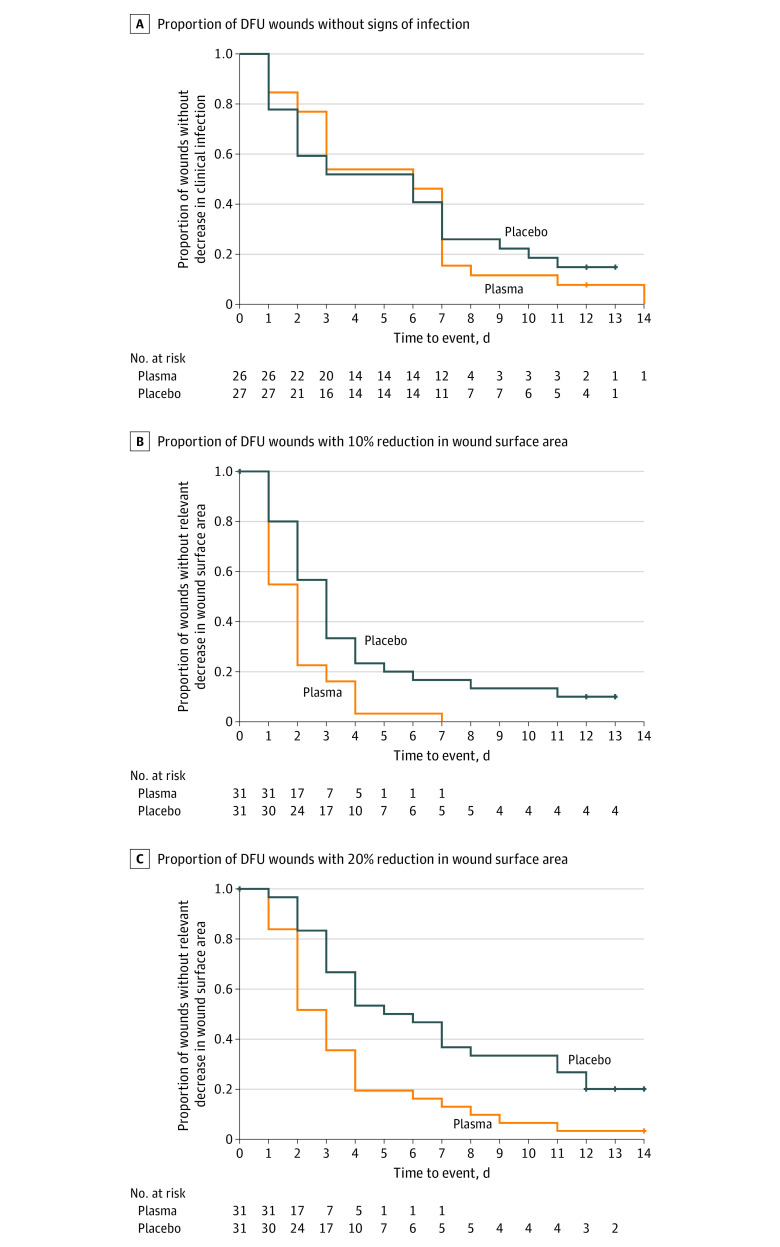
Results: Of 65 diabetic foot ulcer wounds from 45 patients assessed for study, 33 wounds from 29 patients were randomized to CAP and 32 wounds from 28 to placebo, with 62 wounds from 43 patients (31 wounds per group) included for final evaluation (mean [SD] age, 68.5 [9.1] years for full sample). Four patients with 5 wounds of 31 (16.1%) wounds in the CAP group and 3 patients with 4 wounds of 31 (13%) wounds in the placebo group were active smokers. CAP therapy yielded a significant increase in wound healing, both in total mean (SD) area reduction (CAP vs placebo relative units, -26.31 [11.72]; P = .03) and mean (SD) time to relevant wound area reduction (CAP vs placebo relative units, 10% from baseline, 1.60 [0.58]; P = .009). Reduction of infection and microbial load was not significantly different between CAP and placebo. No therapy-related adverse events occurred during therapy; patient's perceptions during therapy were comparable.
Conclusions and relevance: In this randomized clinical trial, CAP therapy resulted in beneficial effects in chronic wound treatment in terms of wound surface reduction and time to wound closure independent from background infection.
Trial registration: ClinicalTrials.gov Identifier: NCT04205942.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
