

Investigating SOFA, delta-SOFA and MPM-III for mortality prediction among critically ill patients at a private tertiary hospital ICU in Kenya: A retrospective cohort study
- PMID: 32673363
- PMCID: PMC7365402
- DOI: 10.1371/journal.pone.0235809
Investigating SOFA, delta-SOFA and MPM-III for mortality prediction among critically ill patients at a private tertiary hospital ICU in Kenya: A retrospective cohort study
Abstract
Background: Outcomes in well-resourced, intensive care units (ICUs) in Kenya are thought to be comparable to those in high-income countries (HICs) but risk-adjusted mortality data is unavailable. We undertook an evaluation of the Aga Khan University Hospital, Nairobi ICU to analyze patient clinical-demographic characteristics, compare the performance of Sequential Organ Failure Assessment (SOFA), delta-SOFA at 48 hours and Mortality Prediction Model-III (MPM-III) mortality prediction systems, and identify factors associated with increased risk of mortality.
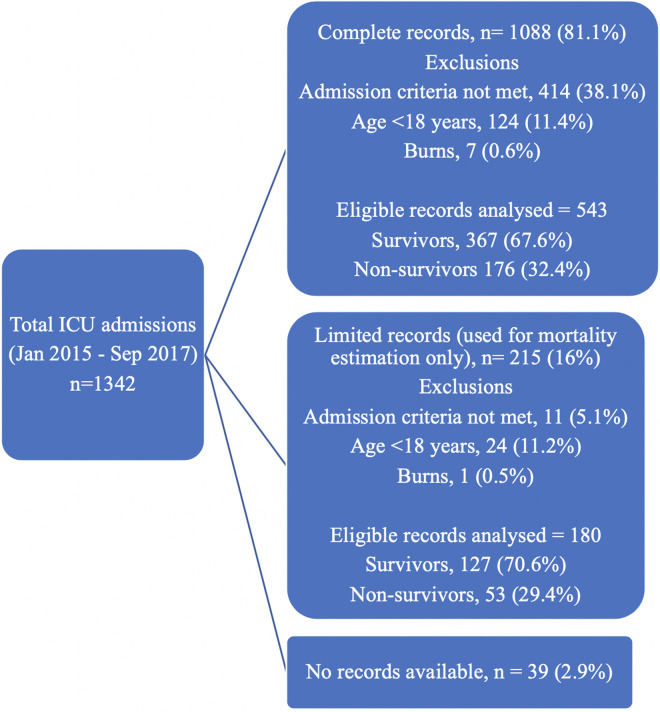
Methods: A retrospective cohort study was conducted of adult patients admitted to the ICU between January 2015 and September 2017. SOFA and MPM-III scores were determined at admission and SOFA repeated at 48 hours.
Results: Approximately 33% of patients did not meet ICU admission criteria. Mortality among the population of critically ill patients in the ICU was 31.7%, most of whom were male (61.4%) with a median age of 53.4 years. High adjusted odds of mortality were found among critically ill patients with leukemia (aOR 6.32, p<0.01), tuberculosis (aOR 3.96, p<0.01), post-cardiac arrest (aOR 3.57, p<0.01), admissions from the step-down unit (aOR 3.13, p<0.001), acute kidney injury (aOR 2.97, p<0.001) and metastatic cancer (aOR 2.45, p = 0.04). The area under the receiver-operating characteristic (ROC) curve of admission SOFA was 0.77 (95% CI, 0.73-0.81), MPM-III 0.74 (95% CI, 0.69-0.79), delta-SOFA 0.69 (95% CI, 0.63-0.75) and 48-hour SOFA 0.83 (95% CI, 0.79-0.87). The difference between SOFA at 48 hours and admission SOFA, MPM-III and delta-SOFA was statistically significant (chi2 = 17.1, 24.2 and 26.5 respectively; p<0.001). Admission SOFA, MPM-III and 48-hour SOFA were well calibrated (p >0.05) while delta-SOFA was borderline (p = 0.05).
Conclusion: Mortality among the critically ill was higher than expected in this well-resourced ICU. 48-hour SOFA performed better than admission SOFA, MPM-III and delta-SOFA in our cohort. While a large proportion of patients did not meet admission criteria but were boarded in the ICU, critically ill patients stepped-up from the step-down unit were unlikely to survive. Patients admitted following a cardiac arrest, and those with advanced disease such as leukemia, stage-4 HIV and metastatic cancer, had particularly poor outcomes. Policies for fair allocation of beds, protocol-driven admission criteria and appropriate case selection could contribute to lowering the risk of mortality among the critically ill to a level on par with HICs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Similar articles
-
Predictors of Survival in Patients with Advanced Gastrointestinal Malignancies Admitted to the Intensive Care Unit.Oncologist. 2019 Apr;24(4):483-490. doi: 10.1634/theoncologist.2018-0328. Epub 2018 Dec 5. Oncologist. 2019. PMID: 30518614 Free PMC article.
-
Acute kidney injury enhances outcome prediction ability of sequential organ failure assessment score in critically ill patients.PLoS One. 2014 Oct 3;9(10):e109649. doi: 10.1371/journal.pone.0109649. eCollection 2014. PLoS One. 2014. PMID: 25279844 Free PMC article.
-
Predicting Mortality in Low-Income Country ICUs: The Rwanda Mortality Probability Model (R-MPM).PLoS One. 2016 May 19;11(5):e0155858. doi: 10.1371/journal.pone.0155858. eCollection 2016. PLoS One. 2016. PMID: 27196252 Free PMC article.
-
Critical care admissions and outcomes in pregnant and postpartum women: a systematic review.Intensive Care Med. 2024 Dec;50(12):1983-1993. doi: 10.1007/s00134-024-07682-3. Epub 2024 Oct 28. Intensive Care Med. 2024. PMID: 39466378
-
Delayed Admission to the Intensive Care Unit and Mortality of Critically Ill Adults: Systematic Review and Meta-analysis.Biomed Res Int. 2022 Feb 7;2022:4083494. doi: 10.1155/2022/4083494. eCollection 2022. Biomed Res Int. 2022. PMID: 35146022 Free PMC article.
Cited by
-
Evaluating the MPM III and SAPS III prognostic models in a war-affected, resource-limited setting: a prospective study from the Gaza Strip.BMC Health Serv Res. 2025 May 6;25(1):646. doi: 10.1186/s12913-025-12833-3. BMC Health Serv Res. 2025. PMID: 40329400 Free PMC article.
-
Performance in mortality prediction of SAPS 3 And MPM-III scores among adult patients admitted to the ICU of a private tertiary referral hospital in Tanzania: a retrospective cohort study.PeerJ. 2021 Nov 16;9:e12332. doi: 10.7717/peerj.12332. eCollection 2021. PeerJ. 2021. PMID: 34820169 Free PMC article.
-
Organisation, staffing and resources of critical care units in Kenya.PLoS One. 2023 Jul 27;18(7):e0284245. doi: 10.1371/journal.pone.0284245. eCollection 2023. PLoS One. 2023. PMID: 37498872 Free PMC article.
-
Granulocyte colony-stimulating factor combined with SOFA score for mortality prediction in patients with sepsis.Medicine (Baltimore). 2024 Dec 27;103(52):e40926. doi: 10.1097/MD.0000000000040926. Medicine (Baltimore). 2024. PMID: 39969364 Free PMC article.
-
EPidemiology, clinical characteristics and Outcomes of 4546 adult admissions to high-dependency and intensive care units in Kenya (EPOK): a multicentre registry-based observational study.Crit Care Explor. 2024 Feb 1;6(2):e1036. doi: 10.1097/CCE.0000000000001036. eCollection 2024 Feb 1. Crit Care Explor. 2024. PMID: 38356864 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
