

Long-Term Outcomes of Patients with Unprotected Left Main Coronary Artery Disease Treated with Percutaneous Angioplasty versus Bypass Grafting: A Meta-Analysis of Randomized Controlled Trials
- PMID: 32674522
- PMCID: PMC7408984
- DOI: 10.3390/jcm9072231
Long-Term Outcomes of Patients with Unprotected Left Main Coronary Artery Disease Treated with Percutaneous Angioplasty versus Bypass Grafting: A Meta-Analysis of Randomized Controlled Trials
Abstract
Background and aim: Treatment of patients with left main coronary artery disease (LMCA) with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) remains controversial. The aim of this meta-analysis was to compare the long-term clinical outcomes of patients with unprotected LMCA treated randomly by PCI or CABG.
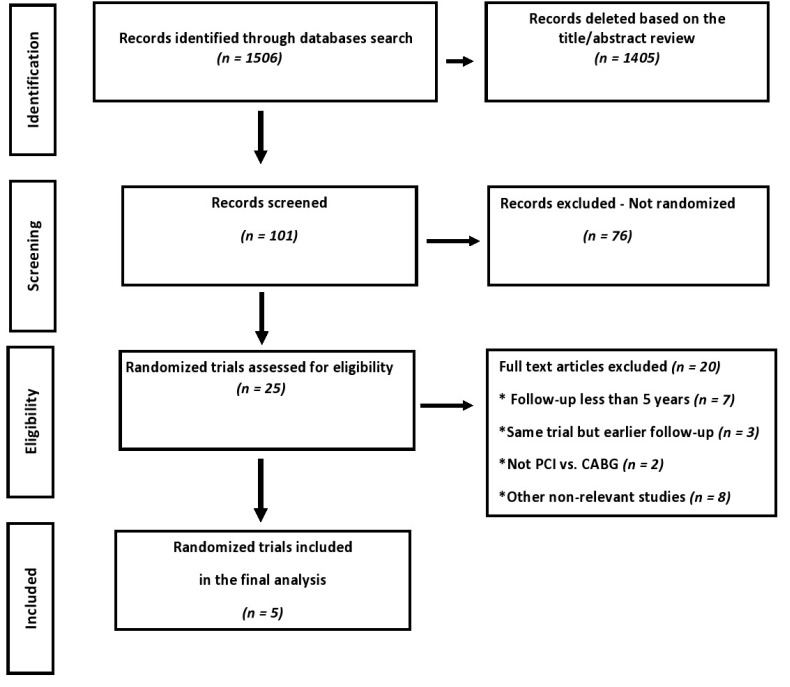
Methods: PubMed, MEDLINE, Embase, Scopus, Google Scholar, CENTRAL and ClinicalTrials.gov database searches identified five randomized trials (RCTs) including 4499 patients with unprotected LMCA comparing PCI (n = 2249) vs. CABG (n = 2250), with a minimum clinical follow-up of five years. Random effect risk ratios were used for efficacy and safety outcomes. The study was registered in PROSPERO. The primary outcome was major adverse cardiac events (MACE), defined as a composite of death from any cause, myocardial infarction or stroke.
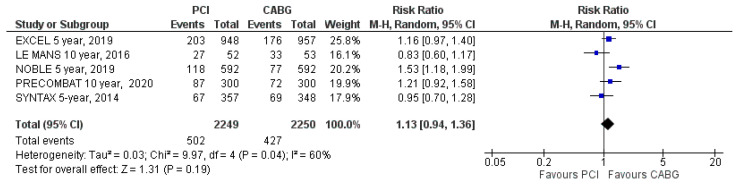
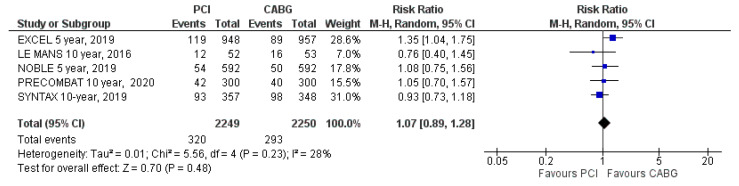
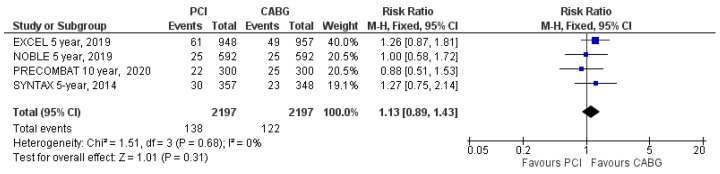
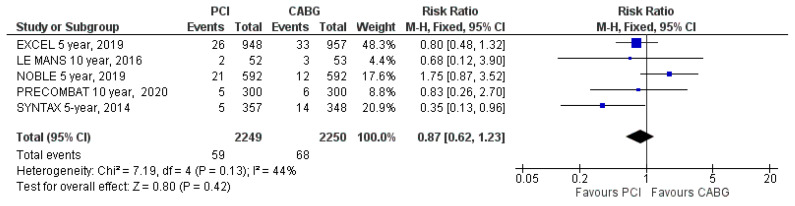
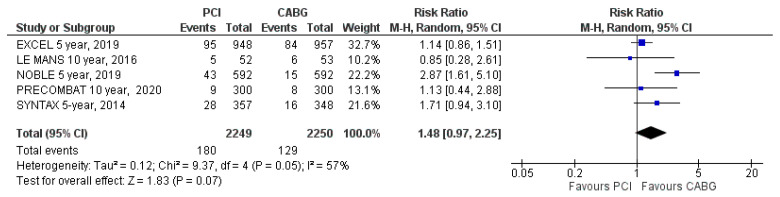
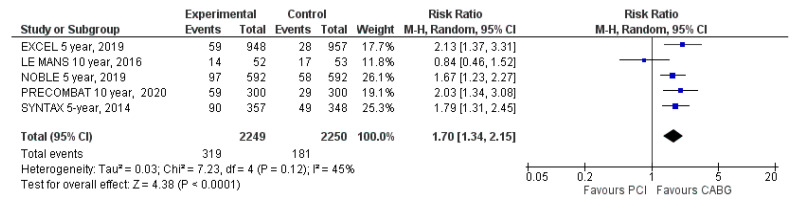
Results: Compared to CABG, patients assigned to PCI had a similar rate of MACE (risk ratio (RR): 1.13; 95% CI: 0.94 to 1.36; p = 0.19), myocardial infarction (RR: 1.48; 95% CI: 0.97 to 2.25; p = 0.07) and stroke (RR: 0.87; 95% CI: 0.62 to 1.23; p = 0.42). Additionally, all-cause mortality (RR: 1.07; 95% CI: 0.89 to 1.28; p = 0.48) and cardiovascular (CV) mortality (RR: 1.13; 95% CI: 0.89 to 1.43; p = 0.31) were not different. However, the risk of any repeat revascularization (RR: 1.70; 95% CI: 1.34 to 2.15; p < 0.00001) was higher in patients assigned to PCI.
Conclusions: The findings of this meta-analysis suggest that the long-term survival and MACE of patients who underwent PCI for unprotected LMCA stenosis were comparable to those receiving CABG, despite a higher rate of repeat revascularization.
Keywords: coronary artery bypass graft; coronary artery disease; percutaneous coronary intervention; unprotected left main.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Patel M.R., Dehmer G.J., Hirshfeld J.W., Smith P.K., Spertus J.A. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 appropriate use criteria for coronary revascularization focused update: A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J. Am. Coll. Cardiol. 2012;59:857–881. doi: 10.1016/j.jacc.2011.12.001. - DOI - PubMed
-
- Holm N.R., Mäkikallio T., Lindsay M.M., Spence M.S., Erglis A., Menown I.B.A., Trovik T., Eskola M., Romppanen H., SYNTAX Extended Survival Investigators et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: Updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020;395:191–199. doi: 10.1016/S0140-6736(19)32972-1. - DOI - PubMed
-
- Thuijs D.J.F.M., Kappetein A.P., Serruys P.W., Mohr F.-W., Morice M.-C., Mack M.J., Holmes D.R., Jr., Curzen N., Davierwala P., SYNTAX Extended Survival Investigators et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394:1325–1334. doi: 10.1016/S0140-6736(19)31997-X. - DOI - PubMed
-
- Stone G.W., Kappetein A.P., Sabik J.F., Pocock S.J., Morice M.C., Puskas J., Kandzari D.E., Karmpaliotis D., Brown W.M., II, EXCEL Trial Investigators et al. Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease. N. Engl. J. Med. 2019;381:1820–1830. doi: 10.1056/NEJMoa1909406. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
