

Endpoints for randomized controlled clinical trials for COVID-19 treatments
- PMID: 32674594
- PMCID: PMC7611901
- DOI: 10.1177/1740774520939938
Endpoints for randomized controlled clinical trials for COVID-19 treatments
Abstract
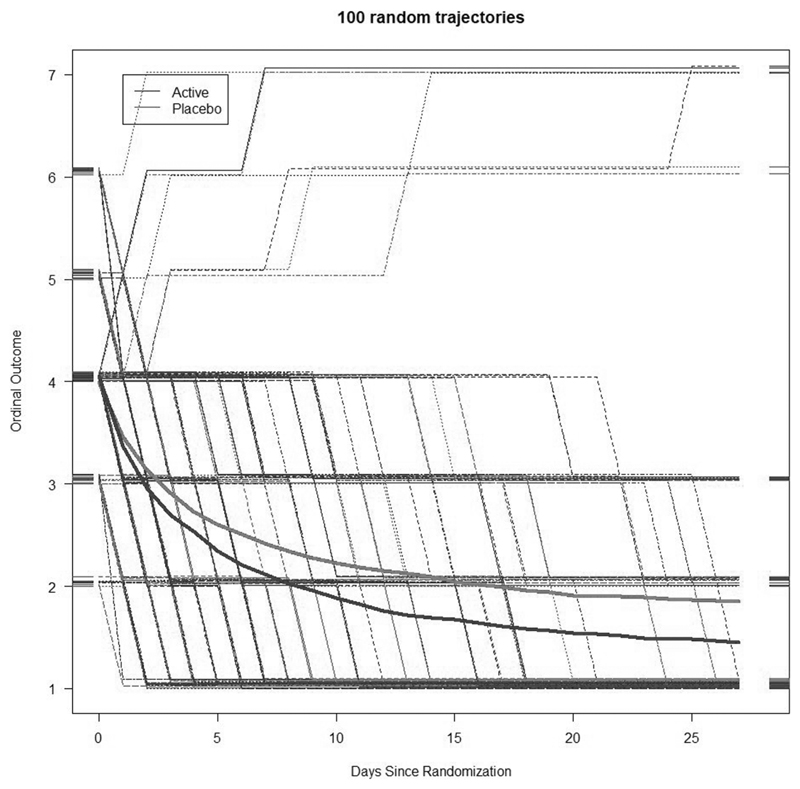
Background: Endpoint choice for randomized controlled trials of treatments for novel coronavirus-induced disease (COVID-19) is complex. Trials must start rapidly to identify treatments that can be used as part of the outbreak response, in the midst of considerable uncertainty and limited information. COVID-19 presentation is heterogeneous, ranging from mild disease that improves within days to critical disease that can last weeks to over a month and can end in death. While improvement in mortality would provide unquestionable evidence about the clinical significance of a treatment, sample sizes for a study evaluating mortality are large and may be impractical, particularly given a multitude of putative therapies to evaluate. Furthermore, patient states in between "cure" and "death" represent meaningful distinctions. Clinical severity scores have been proposed as an alternative. However, the appropriate summary measure for severity scores has been the subject of debate, particularly given the variable time course of COVID-19. Outcomes measured at fixed time points, such as a comparison of severity scores between treatment and control at day 14, may risk missing the time of clinical benefit. An endpoint such as time to improvement (or recovery) avoids the timing problem. However, some have argued that power losses will result from reducing the ordinal scale to a binary state of "recovered" versus "not recovered."
Methods: We evaluate statistical power for possible trial endpoints for COVID-19 treatment trials using simulation models and data from two recent COVID-19 treatment trials.
Results: Power for fixed time-point methods depends heavily on the time selected for evaluation. Time-to-event approaches have reasonable statistical power, even when compared with a fixed time-point method evaluated at the optimal time.
Discussion: Time-to-event analysis methods have advantages in the COVID-19 setting, unless the optimal time for evaluating treatment effect is known in advance. Even when the optimal time is known, a time-to-event approach may increase power for interim analyses.
Keywords: COVID-19; WHO ordinal scale; censoring; clinical trials; endpoints; log-rank test; proportional odds model.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Comment in
-
Lack of harmonization of coronavirus disease ordinal scales.Clin Trials. 2021 Apr;18(2):263-264. doi: 10.1177/1740774520972082. Epub 2020 Dec 15. Clin Trials. 2021. PMID: 33322940 No abstract available.
References
-
- National Institutes of Health. [accessed 12 May 2020];COVID-19 Treatment Guidelines Panel. Coronavirus disease 2019 (COVID-19) treatment guidelines. 2020 https://www.covid19treatmentguidelines.nih.gov/ - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
