

The Effects of ARBs, ACEis, and Statins on Clinical Outcomes of COVID-19 Infection Among Nursing Home Residents
- PMID: 32674818
- PMCID: PMC7294267
- DOI: 10.1016/j.jamda.2020.06.018
The Effects of ARBs, ACEis, and Statins on Clinical Outcomes of COVID-19 Infection Among Nursing Home Residents
Abstract
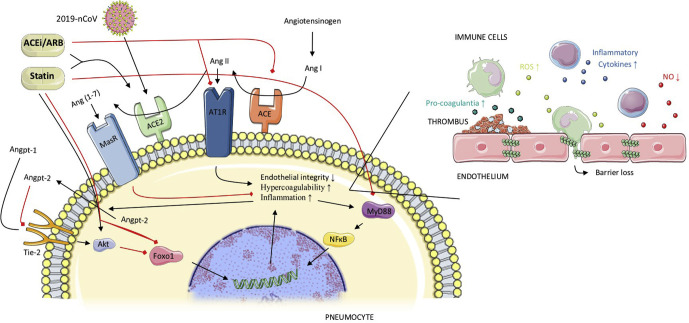
Objectives: Angiotensin-converting enzyme inhibitors (ACEi), angiotensin II receptor blockers (ARBs), and HMG-CoA reductase inhibitors ("statins") have been hypothesized to affect COVID-19 severity. However, up to now, no studies investigating this association have been conducted in the most vulnerable and affected population groups (ie, older adults residing in nursing homes). The objective of this study was to explore the association of ACEi/ARB and/or statins with clinical manifestations in COVID-19-infected older adults residing in nursing homes.
Design: We undertook a retrospective multicenter cohort study to analyze the association between ACEi/ARB and/or statin use with clinical outcome of COVID-19. The outcomes were (1) serious COVID-19 defined as long-stay hospital admission or death within 14 days of disease onset, and (2) asymptomatic (ie, no disease symptoms in the whole study period while still being diagnosed by polymerase chain reaction).
Setting and participants: A total of 154 COVID-19-positive subjects were identified, residing in 1 of 2 Belgian nursing homes that experienced similar COVID-19 outbreaks.
Measures: Logistic regression models were applied with age, sex, functional status, diabetes, and hypertension as covariates.
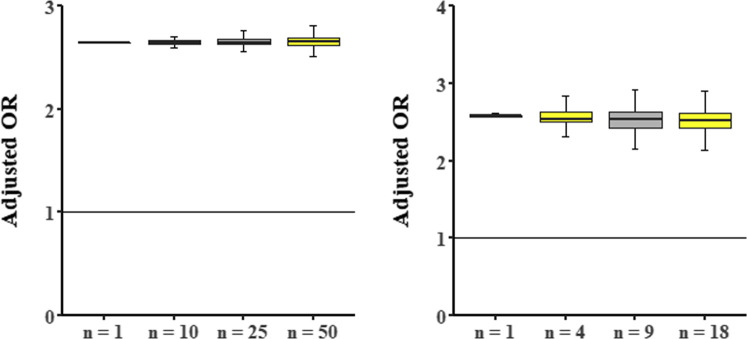
Results: We found a statistically significant association between statin intake and the absence of symptoms during COVID-19 (odds ratio [OR] 2.91; confidence interval [CI] 1.27-6.71), which remained statistically significant after adjusting for covariates (OR 2.65; CI 1.13-6.68). Although the effects of statin intake on serious clinical outcome were in the same beneficial direction, these were not statistically significant (OR 0.75; CI 0.24-1.87). There was also no statistically significant association between ACEi/ARB and asymptomatic status (OR 2.72; CI 0.59-25.1) or serious clinical outcome (OR 0.48; CI 0.10-1.97).
Conclusions and implications: Our data indicate that statin intake in older, frail adults could be associated with a considerable beneficial effect on COVID-19 clinical symptoms. The role of statins and renin-angiotensin system drugs needs to be further explored in larger observational studies as well as randomized clinical trials.
Keywords: Angiotensin-converting enzyme inhibitors; COVID-19; angiotensin II receptor blockers; nursing home residents; statins.
Copyright © 2020 AMDA – The Society for Post-Acute and Long-Term Care Medicine. All rights reserved.
Figures
Comment in
-
Statins and other drugs: Facing COVID-19 as a vascular disease.Pharmacol Res. 2020 Sep;159:105033. doi: 10.1016/j.phrs.2020.105033. Epub 2020 Jun 17. Pharmacol Res. 2020. PMID: 32562814 Free PMC article. No abstract available.
References
-
- Wosten-van Asperen R.M., Bos A.P., Bem R.A. Imbalance between pulmonary angiotensin-converting enzyme and angiotensin-converting enzyme 2 activity in acute respiratory distress syndrome. Pediatr Crit Care Med. 2013;14:E438–E441. - PubMed
-
- Woesten-van Asperen R.M., Lutter R., Specht P.A. Acute respiratory distress syndrome leads to reduced ratio of ACE/ACE2 activities and is prevented by angiotensin-(1–7) or an angiotensin II receptor antagonist. J Pathol. 2011;225:618–627. - PubMed
-
- Jacobson J.R., Barnard J.W., Grigoryev D.N., Ma S.F., Tuder R.M., Garcia J.G. Simvastatin attenuates vascular leak and inflammation in murine inflammatory lung injury. Am J Physiol Lung Cell Mol Physiol. 2005;288:L1026–L1032. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
