

An international, multicenter study of intravenous bevacizumab for bleeding in hereditary hemorrhagic telangiectasia: the InHIBIT-Bleed study
- PMID: 32675221
- PMCID: PMC8327711
- DOI: 10.3324/haematol.2020.261859
An international, multicenter study of intravenous bevacizumab for bleeding in hereditary hemorrhagic telangiectasia: the InHIBIT-Bleed study
Abstract
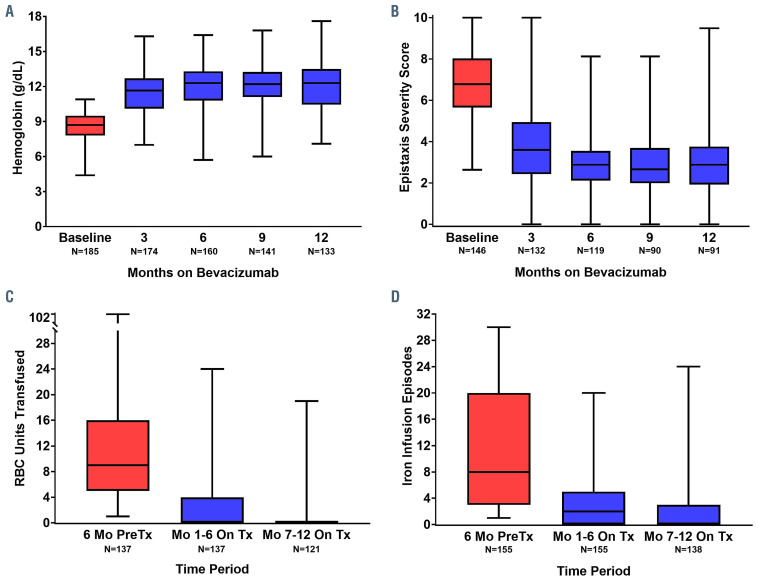
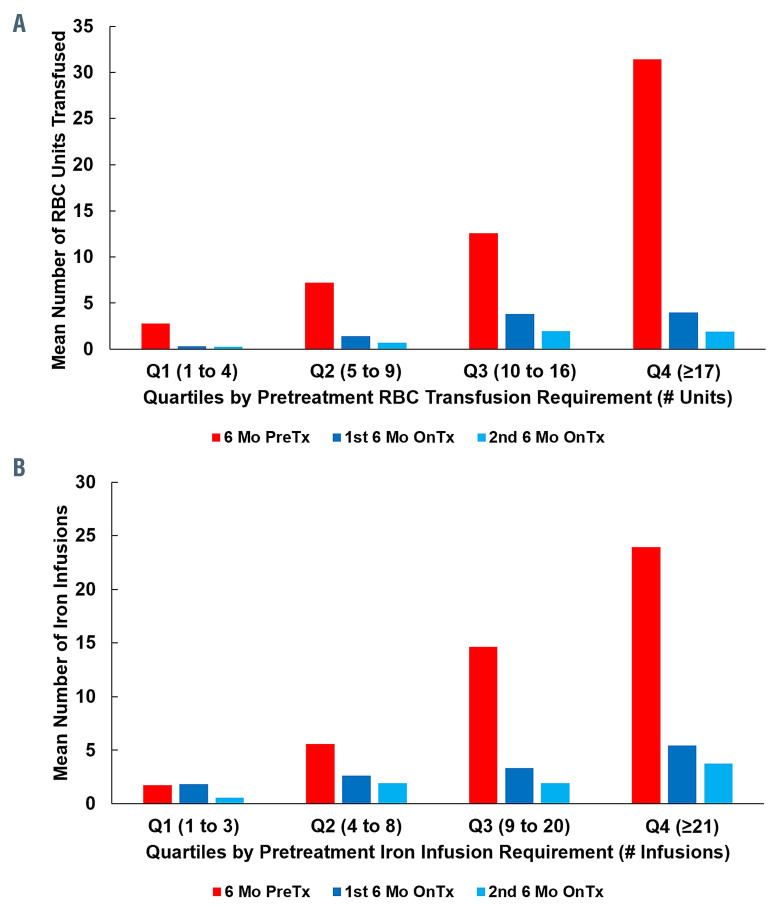
Hereditary hemorrhagic telangiectasia (HHT, Osler-Weber-Rendu disease) is a rare multisystem vascular disorder causing chronic gastrointestinal bleeding, epistaxis, and severe anemia. Bevacizumab, an anti-vascular endothelial growth factor antibody, may be effective to treat bleeding in HHT. This international, multicenter, retrospective study evaluated the use of systemic bevacizumab to treat HHT-associated bleeding and anemia at 12 HHT treatment centers. Hemoglobin, epistaxis severity score, red cell units transfused, and intravenous iron infusions before and after treatment were evaluated using paired means testing and mixed-effects linear models. 238 HHT patients received bevacizumab for a median of 12 (range, 1-96) months. Compared with pretreatment, bevacizumab increased mean hemoglobin by 3.2 g/dL (95% CI, 2.9-3.5 g/dL) [mean hemoglobin 8.6 (8.5, 8.8) g/dL versus 11.8 (11.5, 12.1) g/dL, p<0.0001)] and decreased the epistaxis severity score (ESS) by 3.4 (3.2-3.7) points [mean ESS 6.8 (6.6-7.1) versus 3.4 (3.2-3.7), P<0.0001] during the first year of treatment. Compared with 6 months pretreatment, RBC units transfused decreased by 82% [median of 6.0 (IQR 0.0-13.0) units versus 0 (IQR, 0.0-1.0) units, P<0.0001] and iron infusions decreased by 70% [median of 6.0 (1.0-18.0) infusions versus 1.0 (0.0-4.0) infusions, P<0.0001] during the first 6 months of bevacizumab treatment. Outcomes were similar regardless of underlying pathogenic mutation. Following initial induction infusions, continuous/scheduled bevacizumab maintenance achieved higher hemoglobin and lower ESS than intermittent/as needed maintenance but with more drug exposure. Bevacizumab was well tolerated: hypertension, fatigue, and proteinuria were the most common adverse events. Venous thromboembolism occurred in 2% of patients. In conclusion, systemic bevacizumab was safe and effective to manage chronic bleeding and anemia in HHT.
Figures
References
-
- Fuchizaki U, Miyamori H, Kitagawa S, Kaneko S, Kobayashi K. Hereditary haemorrhagic telangiectasia (Rendu-Osler-Weber disease). Lancet. 2003;362(9394):1490-1494. - PubMed
-
- Kwaan HC, Silverman S. Fibrinolytic activity in lesions of hereditary hemorrhagic telangiectasia. Arch Dermatol. 1973;107(4): 571-573. - PubMed
-
- Watanabe M, Hanawa S, Morishima T. Fibrinolytic activity in cutaneous lesions of hereditary hemorrhagic telangiectasia. Nihon Hifuka Gakkai Zasshi. 1985;95(1):11. - PubMed
-
- Shovlin CL. Hereditary haemorrhagic telangiectasia: pathophysiology, diagnosis and treatment. Blood Rev. 2010;24(6):203-219. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
