

Hospital Volume and Operative Mortality for General Surgery Operations Performed Emergently in Adults
- PMID: 32675542
- PMCID: PMC6803029
- DOI: 10.1097/SLA.0000000000003232
Hospital Volume and Operative Mortality for General Surgery Operations Performed Emergently in Adults
Abstract
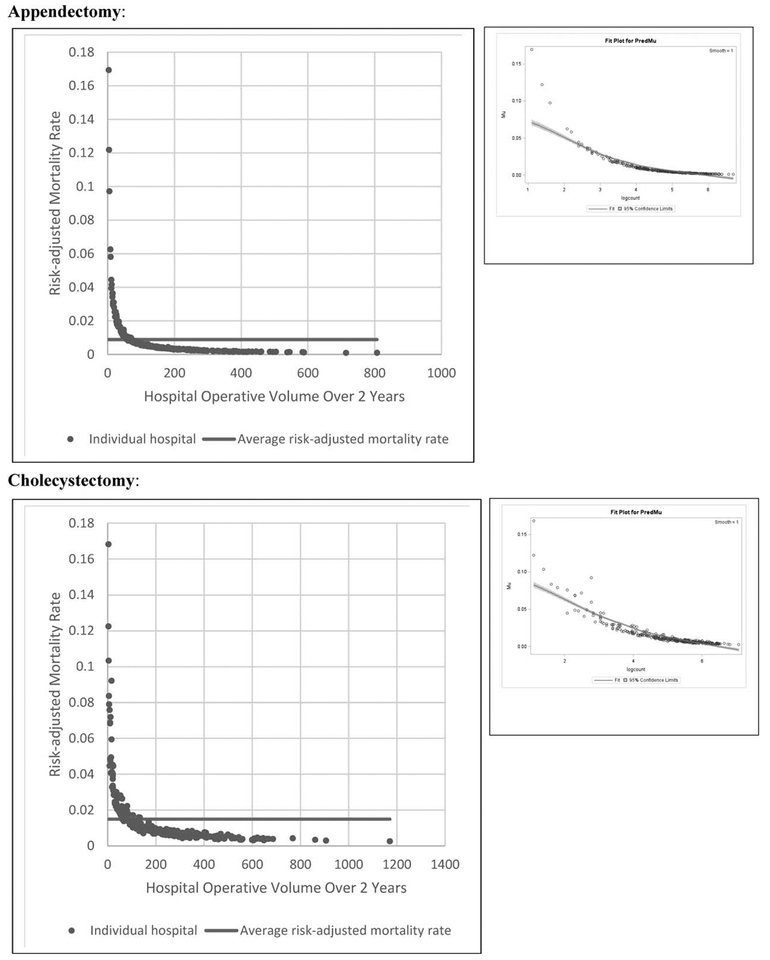
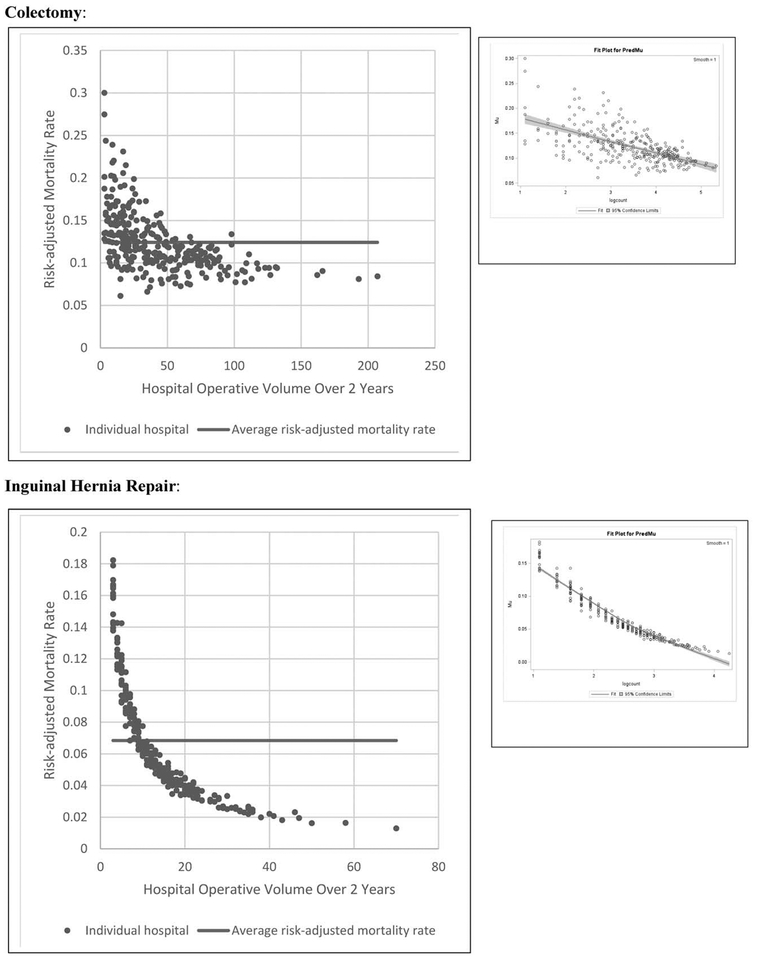
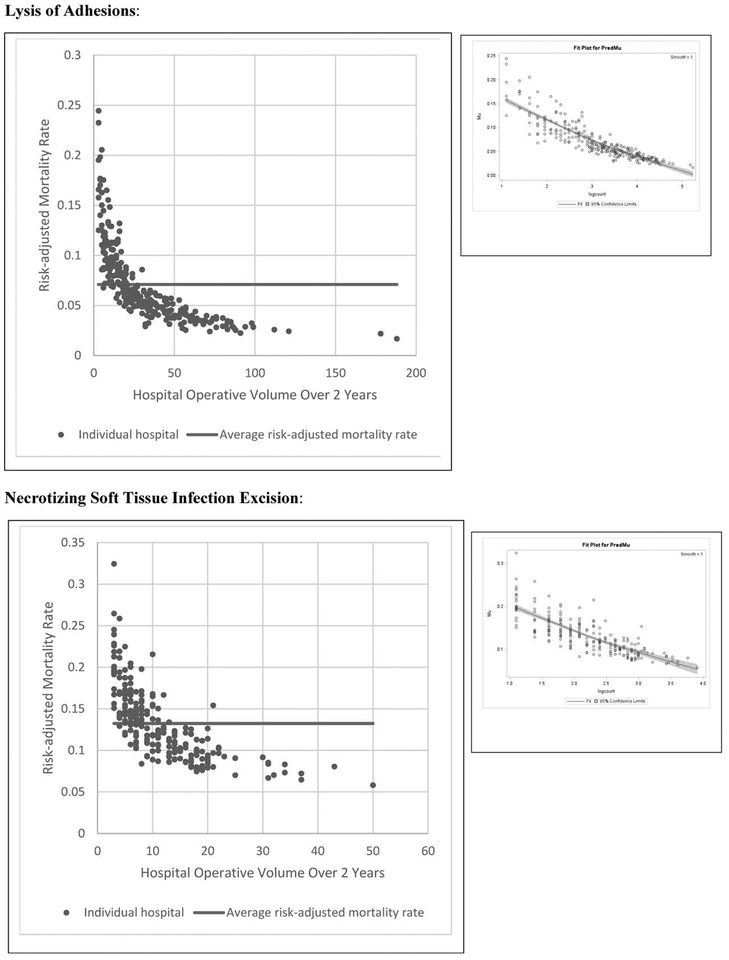
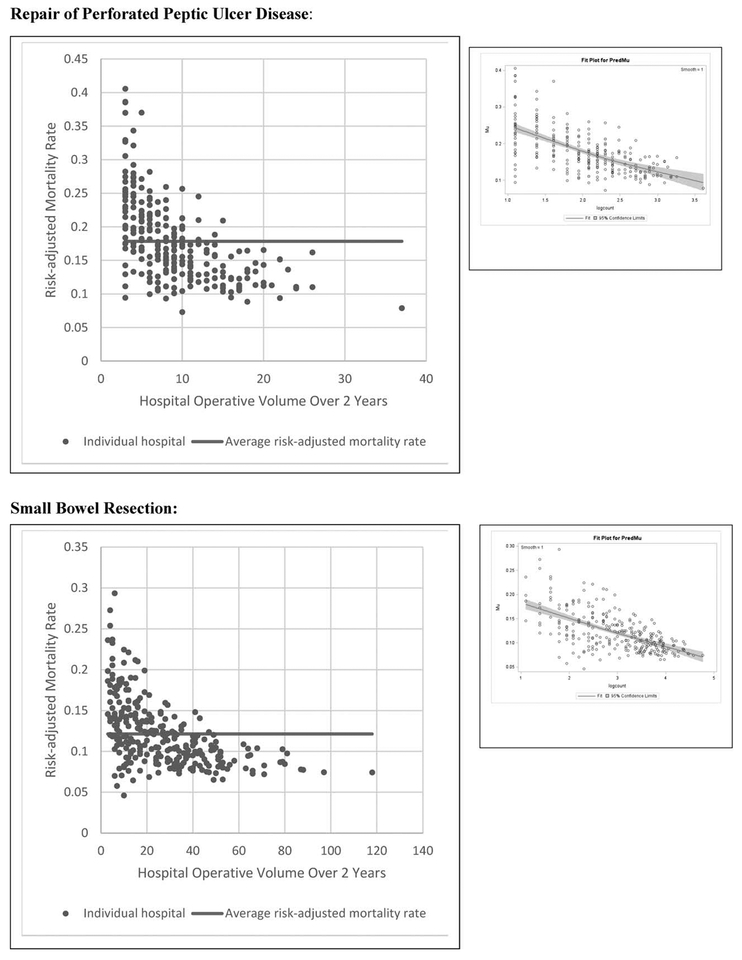
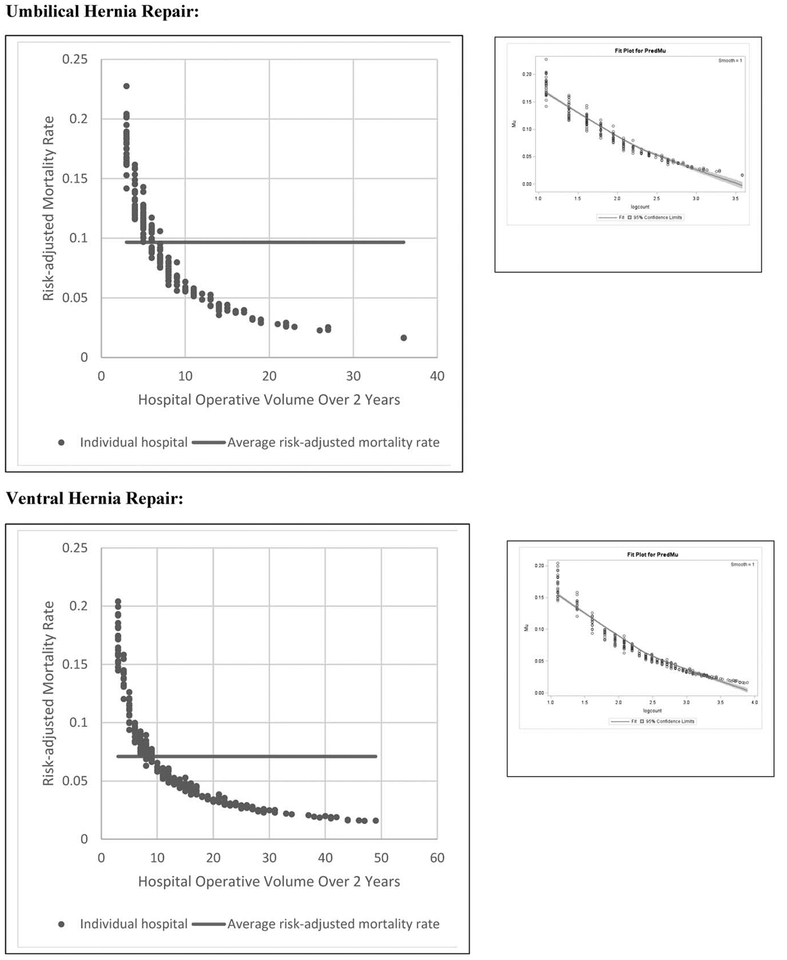
Objective: This study aimed to answer 2 questions: first, to what degree does hospital operative volume affect mortality for adult patients undergoing 1 of 10 common emergency general surgery (EGS) operations? Second, at what hospital operative volume threshold will nearly all patients undergoing an emergency operation realize the average mortality risk?
Background: Nontrauma surgical emergencies are an underappreciated public health crisis in the United States; redefining where such emergencies are managed may improve outcomes. The field of trauma surgery established regionalized systems of care in part because studies demonstrated a clear relationship between hospital volume and survival for traumatic emergencies. Such a relationship has not been well-studied for nontrauma surgical emergencies.
Methods: Retrospective cohort study of all acute care hospitals in California performing nontrauma surgical emergencies. We employed a novel use of an ecological analysis with beta regression to investigate the relationship between hospital operative volume and mortality.
Results: A total of 425 acute care hospitals in California performed 165,123 EGS operations. Risk-adjusted mortality significantly decreased as volume increased for all 10 EGS operations (P < 0.001 for each); the relative magnitude of this inverse relationship differed substantially by procedure. Hospital operative volume thresholds were defined and varied by operation: from 75 cases over 2 years for cholecystectomy to 7 cases for umbilical hernia repair.
Conclusions: Survival rates for nontrauma surgical emergencies were improved when operations were performed at higher-volume hospitals. The use of ecological analysis is widely applicable to the field of surgical outcomes research.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- American College of Surgeons. A growing crisis in patient access to emergency surgical care. Bull Am Coll Surg. 2006;91:8–19. - PubMed
-
- Trunkey DD. A growing crisis in patient access to emergency care: a different interpretation and alternative solutions. Bull Am Coll Surg. 2006;91:12–22. - PubMed
-
- Gale SC, Shafi S, Dombrovskiy VY, et al. The public health burden of emergency general surgery in the United States: a 10-year analysis of the Nationwide Inpatient Sample—2001 to 2010. J Trauma Acute Care Surg. 2014;77:202–208. - PubMed
-
- Acute Care Congress. Acute care congress on the future of emergency surgical care in the United States. J Trauma. 2009;67:1–7. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
