

Controversies and challenges in the histologic subtyping of lung adenocarcinoma
- PMID: 32676350
- PMCID: PMC7354137
- DOI: 10.21037/tlcr.2019.12.30
Controversies and challenges in the histologic subtyping of lung adenocarcinoma
Abstract
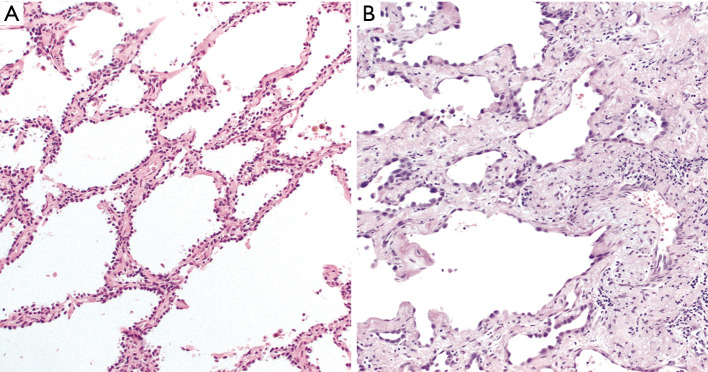
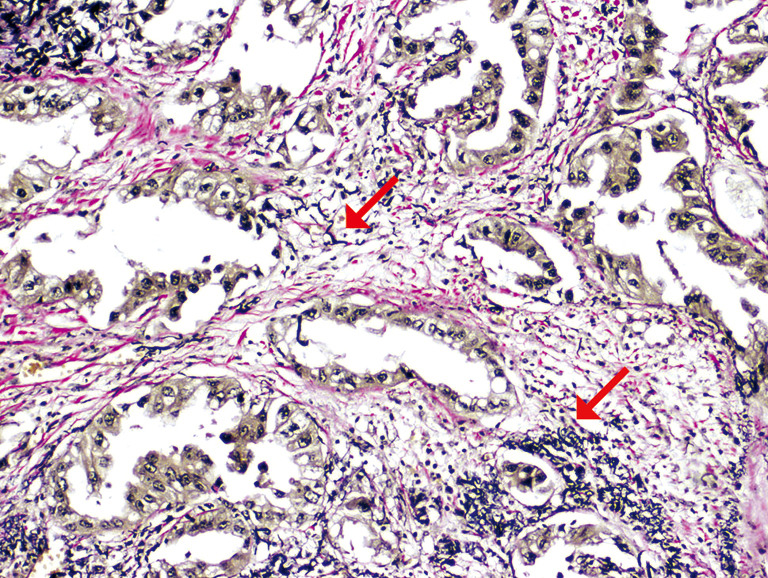
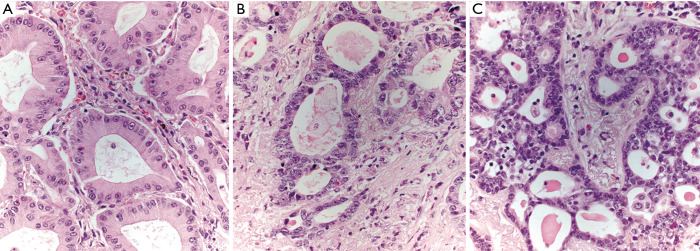
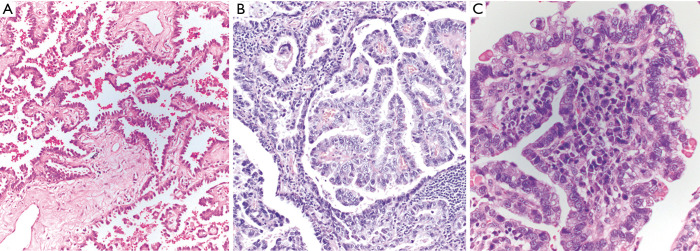
Lung adenocarcinomas differ in prognosis based on their histologic growth pattern. Adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA) both have an excellent prognosis when completely resected, whereas solid and micropapillary-predominant adenocarcinomas do not, with other patterns falling in between. In recent years, it has become apparent that even within histologic patterns, there are differences in appearance that are clinically important, such as complex acinar formations and highly variable-sized papillae. This review highlights prognostically important histologic features in lung adenocarcinoma that have emerged since implementation of the current World Health Organization (WHO) classification of lung adenocarcinoma.
Keywords: Lung adenocarcinoma; classification; histologic; pathology; subtyping.
2020 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The author has completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tlcr.2019.12.30). The series “Selected Highlights of the 2019 Pulmonary Pathology Society Biennial Meeting” was commissioned by the editorial office without any sponsorship or funding. The author has no other conflicts of interest to declare.
Figures

References
-
- Travis WD, Brambilla E, Noguchi M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol 2011;6:244-85. 10.1097/JTO.0b013e318206a221 - DOI - PMC - PubMed
-
- Travis WD, Brambilla E, Burke AP, et al. editors. WHO classification of Tumours of Lung Pleura, Thymus and Heart. 4th ed. Lyon: IARC, 2015. - PubMed
-
- Boland JM, Froemming AT, Wampfler JA, et al. Adenocarcinoma in situ, minimally invasive adenocarcinoma, and invasive pulmonary adenocarcinoma-analysis of interobserver agreement, survival, radiographic characteristics, and gross pathology in 296 nodules. Hum Pathol 2016;51:41-50. 10.1016/j.humpath.2015.12.010 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources