

Clinical utility of chest radiography for severe COVID-19
- PMID: 32676371
- PMCID: PMC7358410
- DOI: 10.21037/qims-20-642
Clinical utility of chest radiography for severe COVID-19
Abstract
Background: Chest radiography (CXR) is performed more widely and readily than CT for the management of coronavirus disease (COVID-19), but there remains little data on its clinical utility. This study aims to assess the diagnostic performance of CXR, with emphasis on its predictive value, for severe COVID-19 disease.
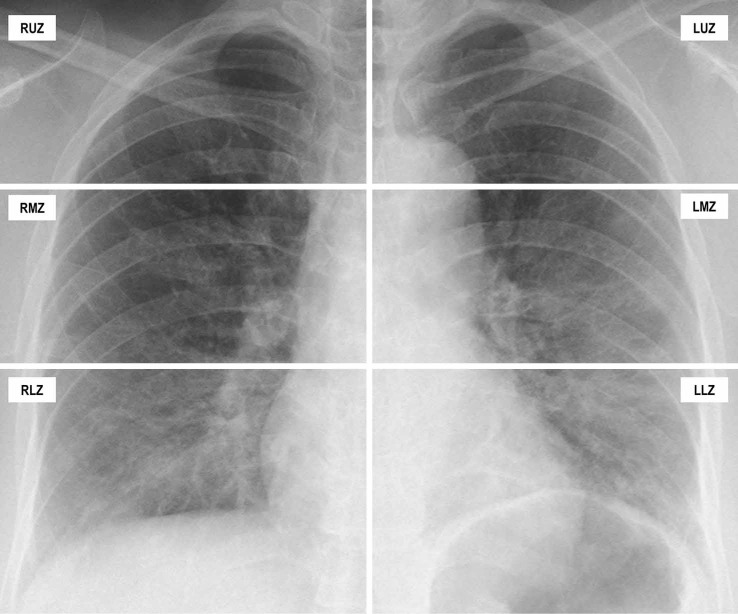
Methods: A retrospective cohort study was conducted, 358 chest radiographs were performed on 109 COVID-19 patients (median age 44.4 years, 58 males and 30 with comorbidities) admitted between 22 January 2020 and 15 March 2020. Each CXR was reviewed and scored by three radiologists in consensus using a 72-point COVID-19 Radiographic Score (CRS). Disease severity was determined by the need for supplemental oxygen and mechanical ventilation.
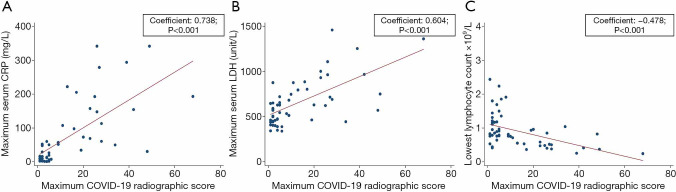
Results: Patients who needed supplemental oxygen (n=19, 17.4%) were significantly older (P<0.001) and significantly more of them had co-morbidities (P=0.011). They also had higher C-reactive protein (CRP) (P<0.001), higher lactate dehydrogenase (LDH) (P<0.001), lower lymphocyte count (P<0.001) and lower hemoglobin (Hb) (P=0.001). Their initial (CRSinitial) and maximal CRS (CRSmax) were higher (P<0.001). Adjusting for age and baseline hemoglobin, the AUROC of CRSmax (0.983) was as high as CRPmax (0.987) and higher than the AUROC for lymphocyte countmin (0.897), and LDHmax (0.900). The AUROC for CRSinitial was slightly lower (0.930). CRSinitial ≥5 had a sensitivity of 63% and specificity of 92% in predicting the need for oxygen, and 73% sensitivity and 88% specificity in predicting the need for mechanical ventilation. CRS between the 6th and 10th day from the onset of symptoms (CRSD6-10) ≥5 had a sensitivity of 89% and specificity of 95% in predicting the need for oxygen, and 100% sensitivity and 86% specificity in predicting the need for mechanical ventilation.
Conclusions: Adjusting for key confounders of age and baseline Hb, CRSmax performed comparable to or better than laboratory markers in the diagnosis of severe disease. CXR performed between the 6th and 10th days from symptom onset was a better predictor of severe disease than CXR performed earlier at presentation. A benign clinical course was seen in CXR that were normal or had very mild abnormalities.
Keywords: Radiography; pneumonia; thoracic; viruses.
2020 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/qims-20-642). The authors have no conflicts of interest to declare.
Figures
References
-
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W, China Novel Coronavirus Investigating and Research Team A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med 2020;382:727-33. 10.1056/NEJMoa2001017 - DOI - PMC - PubMed
-
- World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report.—91. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/2...
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous