

Effect of Interleukin-17 in the Activation of Monocyte Subsets in Patients with ST-Segment Elevation Myocardial Infarction
- PMID: 32676508
- PMCID: PMC7336211
- DOI: 10.1155/2020/5692829
Effect of Interleukin-17 in the Activation of Monocyte Subsets in Patients with ST-Segment Elevation Myocardial Infarction
Abstract
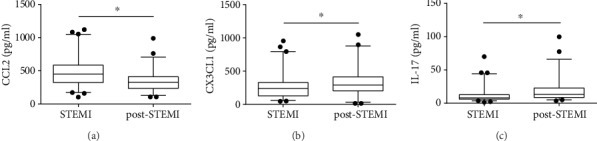
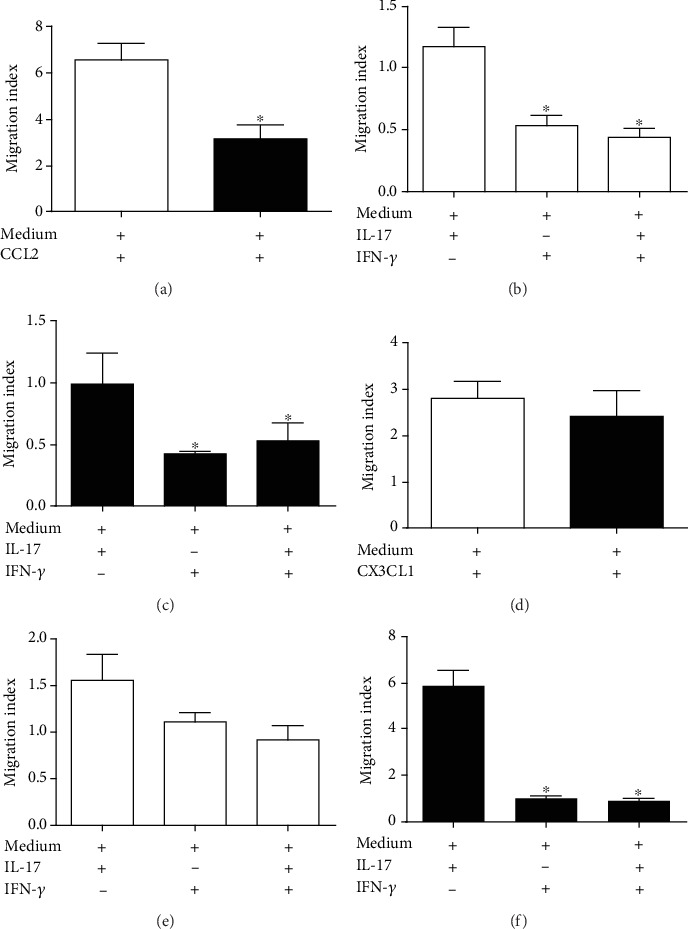
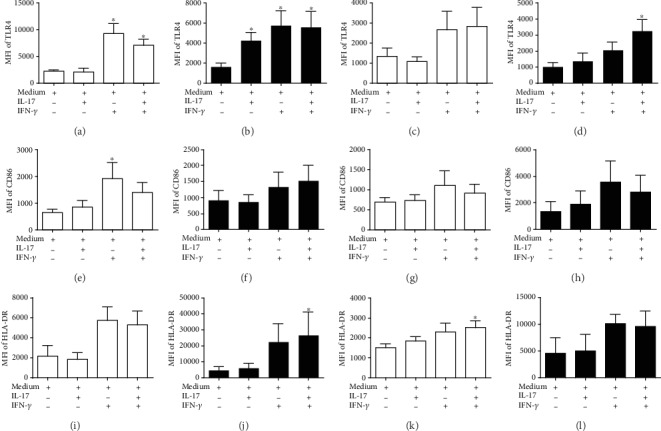
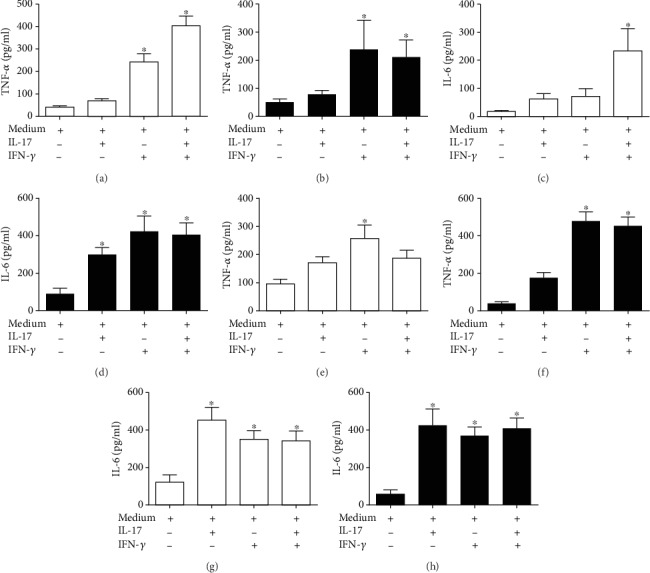
Interleukin- (IL-) 17 is increased in acute myocardial infarction (AMI) and plays a key role in inflammatory diseases through its involvement in the activation of leukocytes. Here, we describe for the first time the effect of IL-17 in the migration and activation of monocyte subsets in patients during ST-segment elevation myocardial infarction (STEMI) and post-STEMI. We analyzed the circulating levels of IL-17 in patient plasma. A gradual increase in IL-17 was found in STEMI and post-STEMI patients. Additionally, IL-17 had a powerful effect on the recruitment of CD14++CD16+/CD14+CD16++ monocytes derived from patients post-STEMI compared with the monocytes from patients with STEMI, suggesting that IL-17 recruits monocytes with inflammatory activity post-STEMI. Furthermore, IL-17 increased the expression of TLR4 on CD14 + CD16 - and CD14++CD16+/CD14+CD16++ monocytes post-STEMI and might enhance the response to danger-associated molecular patterns post-STEMI. Moreover, IL-17 induced secretion of IL-6 from CD14++CD16- and CD14++CD16+/CD14+CD16++ monocytes both in STEMI and in post-STEMI, which indicates that IL-17 has an effect on the secretion of proinflammatory cytokines from monocytes during STEMI and post-STEMI. Overall, we demonstrate that in STEMI and post-STEMI, IL-17 is increased and induces the migration and activation of monocyte subsets, possibly contributing to the inflammatory response through TLR4 and IL-6 secretion.
Copyright © 2020 Montserrat Guadalupe Garza-Reyes et al.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures
References
-
- Tsujioka H., Imanishi T., Ikejima H., et al. Impact of heterogeneity of human peripheral blood monocyte subsets on myocardial salvage in patients with primary acute myocardial infarction. Journal of the American College of Cardiology. 2009;54(2):130–138. doi: 10.1016/j.jacc.2009.04.021. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
