

This is a preprint.
Mapping Systemic Inflammation and Antibody Responses in Multisystem Inflammatory Syndrome in Children (MIS-C)
- PMID: 32676612
- PMCID: PMC7359537
- DOI: 10.1101/2020.07.04.20142752
Mapping Systemic Inflammation and Antibody Responses in Multisystem Inflammatory Syndrome in Children (MIS-C)
Update in
-
Mapping Systemic Inflammation and Antibody Responses in Multisystem Inflammatory Syndrome in Children (MIS-C).Cell. 2020 Nov 12;183(4):982-995.e14. doi: 10.1016/j.cell.2020.09.034. Epub 2020 Sep 14. Cell. 2020. PMID: 32991843 Free PMC article.
Abstract
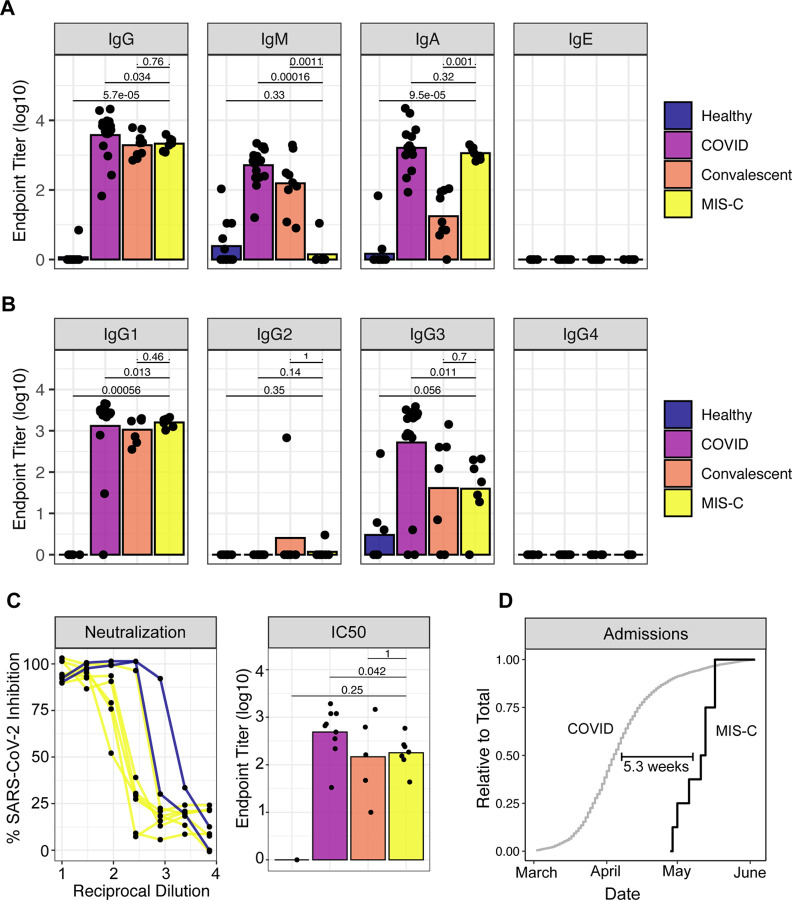
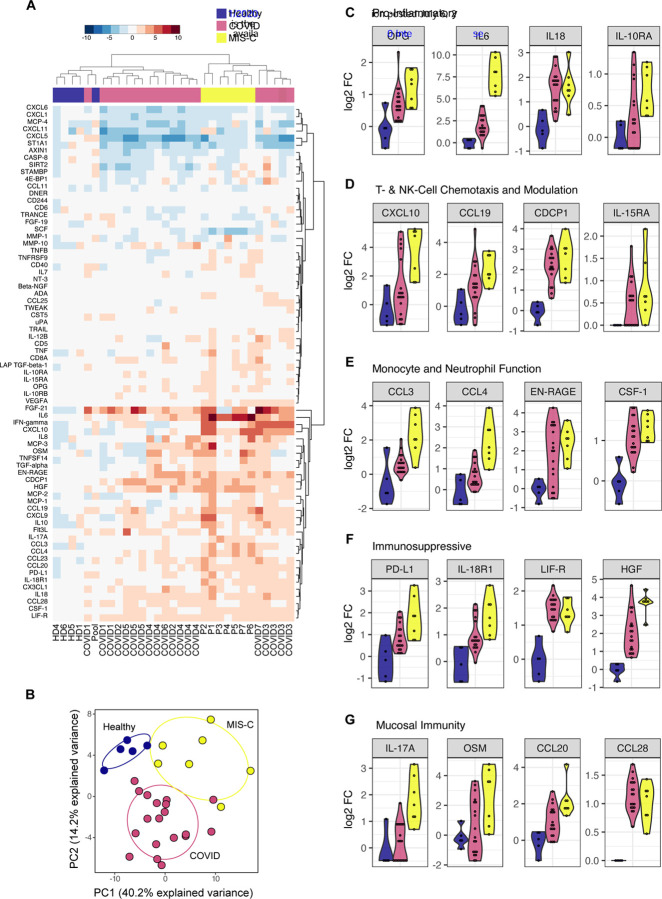
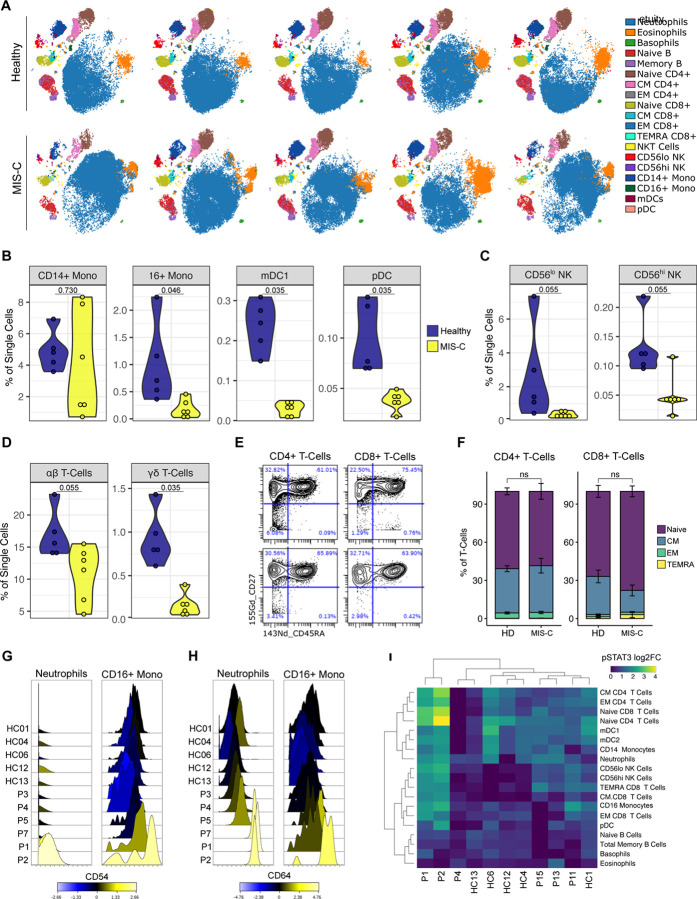
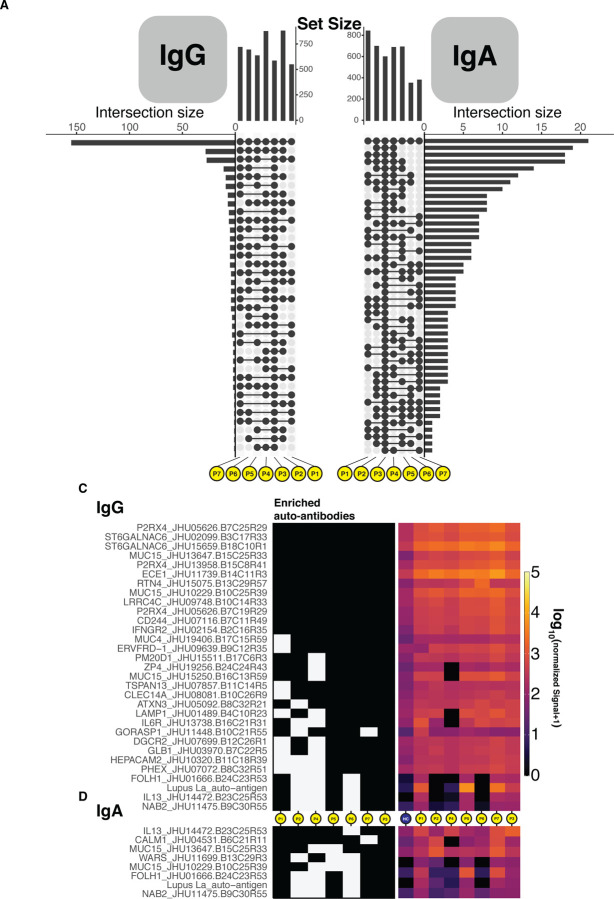
Initially, the global outbreak of COVID-19 caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spared children from severe disease. However, after the initial wave of infections, clusters of a novel hyperinflammatory disease have been reported in regions with ongoing SARS-CoV-2 epidemics. While the characteristic clinical features are becoming clear, the pathophysiology remains unknown. Herein, we report on the immune profiles of eight Multisystem Inflammatory Syndrome in Children (MIS-C) cases. We document that all MIS-C patients had evidence of prior SARS-CoV-2 exposure, mounting an antibody response with normal isotype-switching and neutralization capability. We further profiled the secreted immune response by high-dimensional cytokine assays, which identified elevated signatures of inflammation (IL-18 and IL-6), lymphocytic and myeloid chemotaxis and activation (CCL3, CCL4, and CDCP1) and mucosal immune dysregulation (IL-17A, CCL20, CCL28). Mass cytometry immunophenotyping of peripheral blood revealed reductions of mDC1 and non-classical monocytes, as well as both NK- and T- lymphocytes, suggesting extravasation to affected tissues. Markers of activated myeloid function were also evident, including upregulation of ICAM1 and FcγR1 in neutrophil and non-classical monocytes, well-documented markers in autoinflammation and autoimmunity that indicate enhanced antigen presentation and Fc-mediated responses. Finally, to assess the role for autoimmunity secondary to infection, we profiled the auto-antigen reactivity of MIS-C plasma, which revealed both known disease-associated autoantibodies (anti-La) and novel candidates that recognize endothelial, gastrointestinal and immune-cell antigens. All patients were treated with anti-IL6R antibody or IVIG, which led to rapid disease resolution tracking with normalization of inflammatory markers.
Keywords: COVID19; Kawasaki-like; MIS-C; PIMS; SARS-CoV-2; autoimmunity; dysfunction; immune; pediatrics.
Conflict of interest statement
Declaration of Interests DB reports ownership in Lab11 Therapeutics. S.G. reports consultancy and/or advisory roles for Merck, Neon Therapeutics and OncoMed and research funding from Bristol-Myers Squibb, Genentech, Immune Design, Agenus, Janssen R&D, Pfizer, Takeda, and Regeneron.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous