

Preservation of optic nerve structure by complement inhibition in experimental glaucoma
- PMID: 32676862
- PMCID: PMC8285355
- DOI: 10.1007/s00441-020-03240-7
Preservation of optic nerve structure by complement inhibition in experimental glaucoma
Erratum in
-
Correction to: Preservation of optic nerve structure by complement inhibition in experimental glaucoma.Cell Tissue Res. 2021 Oct;386(1):205. doi: 10.1007/s00441-021-03501-z. Cell Tissue Res. 2021. PMID: 34487235 Free PMC article. No abstract available.
Abstract
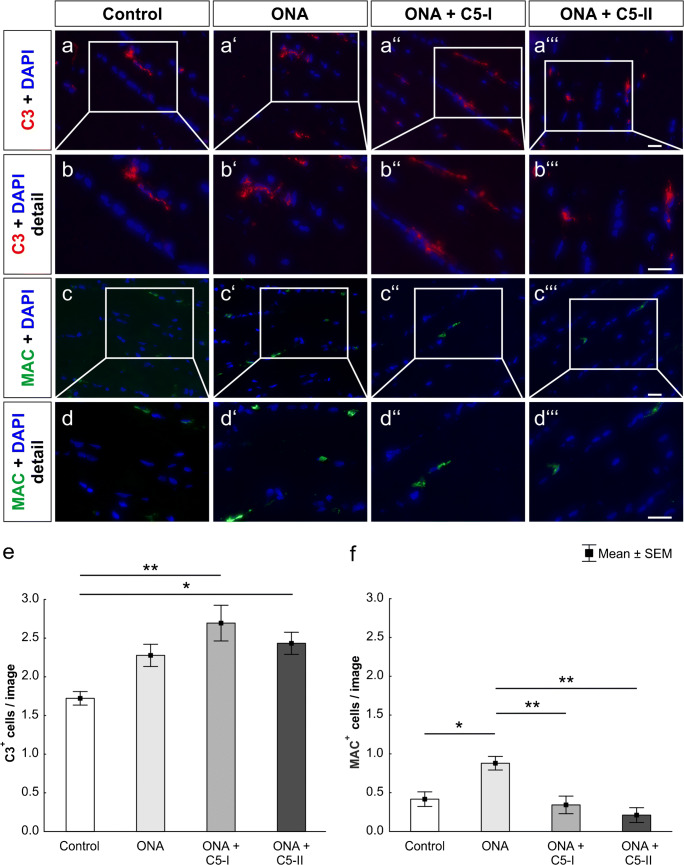
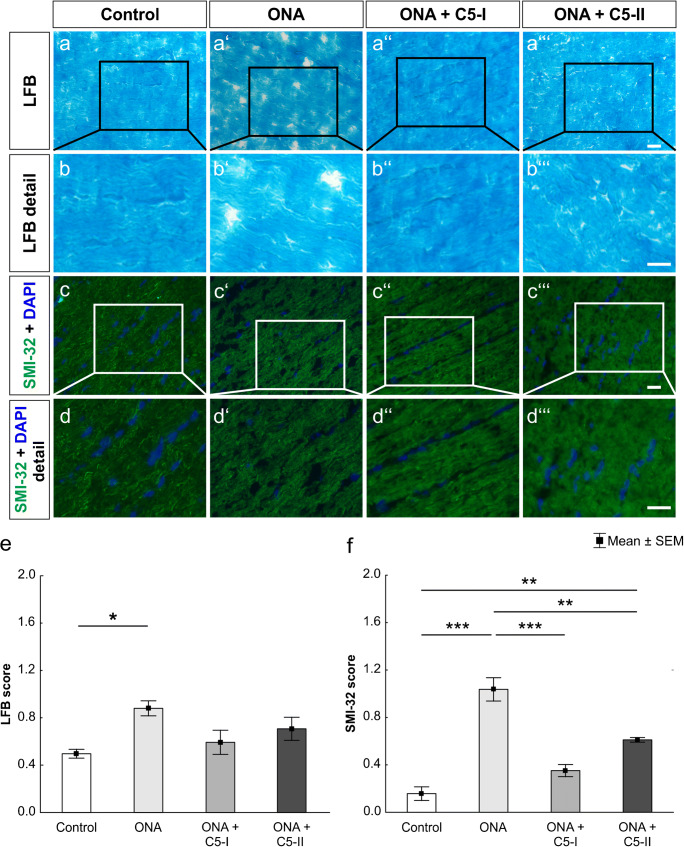
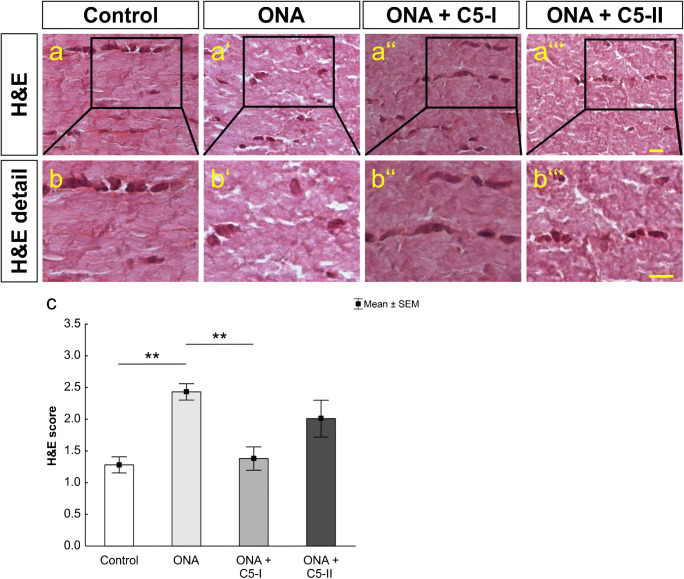
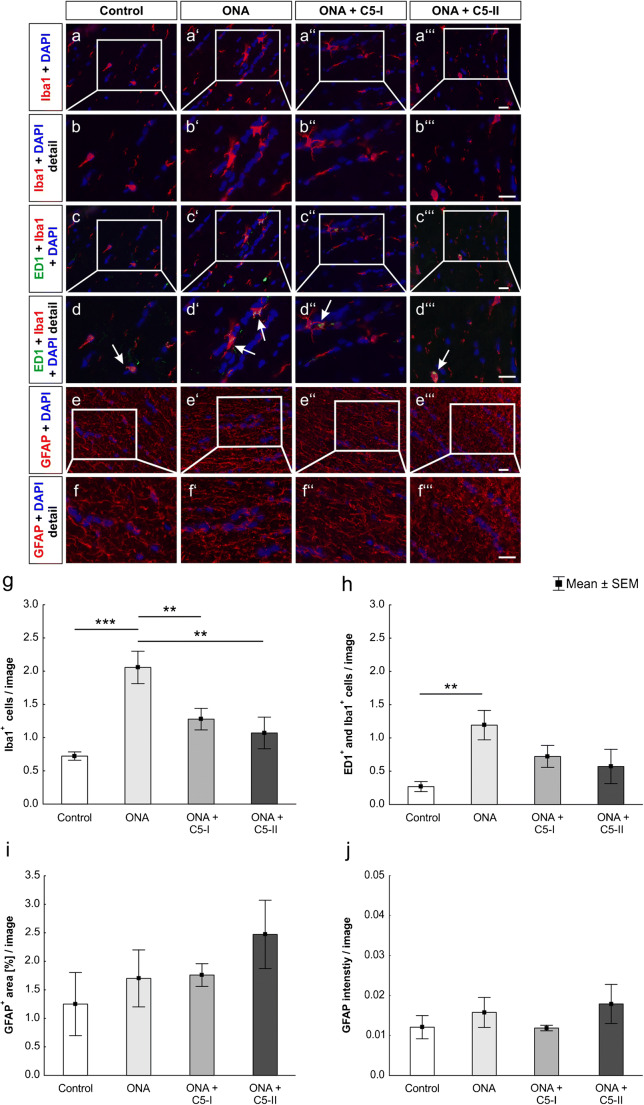
Glaucoma is characterized by a progressive damage of the retina and the optic nerve. Despite a huge research interest, the exact pathomechanisms are still unknown. In the experimental autoimmune glaucoma model, rats develop glaucoma-like damage of the retina and the optic nerve after immunization with an optic nerve antigen homogenate (ONA). An early activation of the complement system, even before optic nerve degeneration, was reported in this model. Here, we investigated the effects of a monoclonal antibody against complement factor C5 on optic nerves. Rats were immunized with ONA and compared to controls. In one eye of some ONA animals, the antibody against C5 was intravitreally injected (15 μmol: ONA + C5-I or 25 μmol: ONA + C5-II) before immunization and then every 2 weeks. After 6 weeks, optic nerves were processed for histology (n = 6/group). These analyses demonstrated that the intravitreal therapy reduced the depositions of the membrane attack complex compared to ONA animals (ONA + C5-I: p = 0.005; ONA + C5-II: p = 0.002). Cellular infiltration was significantly reduced in the ONA + C5-I group (p = 0.003), but not in ONA + C5-II tissues (p = 0.41). Furthermore, SMI-32 staining revealed that neurofilament was preserved in both treatment groups compared to ONA optic nerves (both p = 0.002). A decreased amount of microglia was found in treated animals in comparison to the ONA group (ONA + C5-I: p = 0.03; ONA + C5-II: p = 0.009). We observed, for the first time, that a complement system inhibition could prevent optic nerve damage in an autoimmune glaucoma model. Therefore, complement inhibition could serve as a new therapeutic tool for glaucoma.
Keywords: Complement inhibition; Complement system; Glaucoma; Microglia; Optic nerve.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Becker S, Reinehr S, Dick HB, Joachim SC (2015) Complement activation after induction of ocular hypertension in an animal model. Ophthalmologe 112:41–48 - PubMed
-
- Boehm N, Wolters D, Thiel U, Lossbrand U, Wiegel N, Pfeiffer N, Grus FH (2012) New insights into autoantibody profiles from immune privileged sites in the eye: a glaucoma study. Brain Behav Immun 26:96–102 - PubMed
-
- Bonomi L, Marchini G, Marraffa M, Bernardi P, De Franco I, Perfetti S, Varotto A, Tenna V (1998) Prevalence of glaucoma and intraocular pressure distribution in a defined population. The Egna-Neumarkt Study Ophthalmology 105:209–215 - PubMed
-
- Bosco A, Inman DM, Steele MR, Wu G, Soto I, Marsh-Armstrong N, Hubbard WC, Calkins DJ, Horner PJ, Vetter ML (2008) Reduced retina microglial activation and improved optic nerve integrity with minocycline treatment in the DBA/2J mouse model of glaucoma. Invest Ophthalmol Vis Sci 49:1437–1446 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
