

Risk to health from COVID-19 for anaesthetists and intensivists - a narrative review
- PMID: 32677708
- PMCID: PMC7405109
- DOI: 10.1111/anae.15220
Risk to health from COVID-19 for anaesthetists and intensivists - a narrative review
Abstract
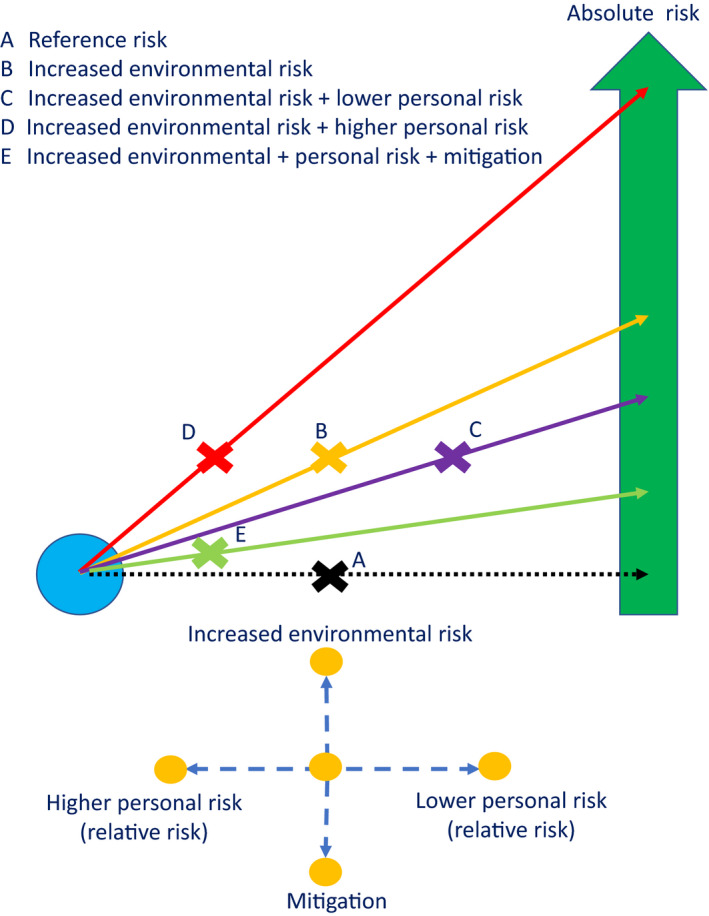
Healthcare workers are at an increased risk of infection, harm and death from COVID-19. Close and prolonged exposure to individuals infectious with SARS-CoV-2 leads to infection. A person's individual characteristics (age, sex, ethnicity and comorbidities) then influence the subsequent risk of COVID-19 leading to hospitalisation, critical care admission or death. While relative risk is often reported as a measure of individual danger, absolute risk is more important and dynamic, particularly in the healthcare setting. Individual risk interacts with exposure and environmental risk-factors, and the extent of mitigation to determine overall risk. Hospitals are a unique environment in which there is a significantly increased risk of infection for all healthcare workers. Anaesthetists and intensivists particularly are at high risk of exposure to SARS-CoV-2 infected patients due to their working environments and exposure to certain patient groups. However, the available evidence suggests that the risk for this group of individuals is not currently increased. This review examines factors associated with increased risk of infection with SARS-CoV-2, increasing severity of COVID-19 and death. A risk tool is proposed that includes personal, environmental and mitigating factors, and enables an individualised dynamic 'point-of-time' risk assessment.
Keywords: COVID-19; healthcare worker; intensive care; mortality; pandemic; risk.
© 2020 The Association of Anaesthetists.
Figures
Comment in
-
Aerosols: are anaesthetists at risk of COVID-19 or not?Anaesthesia. 2021 Mar;76 Suppl 3:19-20. doi: 10.1111/anae.15334. Epub 2020 Dec 8. Anaesthesia. 2021. PMID: 33616896 No abstract available.
References
-
- Public Health England . Transmission characteristics and principles of infection prevention and control. https://www.gov.uk/government/publications/wuhan‐novel‐coronavirus‐infec... (accessed 29/06/2020).
-
- Wölfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID‐2019. Nature 2020; 581: 465–9. - PubMed
-
- Cook TM. Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic ‐ a narrative review. Anaesthesia 2020; 75: 920–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
