

Clinical characteristics and management of primary mediastinal cysts: A single-center experience
- PMID: 32677753
- PMCID: PMC7471030
- DOI: 10.1111/1759-7714.13555
Clinical characteristics and management of primary mediastinal cysts: A single-center experience
Abstract
Background: In this study we aimed to assess the clinical outcomes of performing video-assisted thoracic surgery (VATS) to treat primary mediastinal cysts (PMCs) and investigate the clinical factors which increase the difficulties associated with VATS.
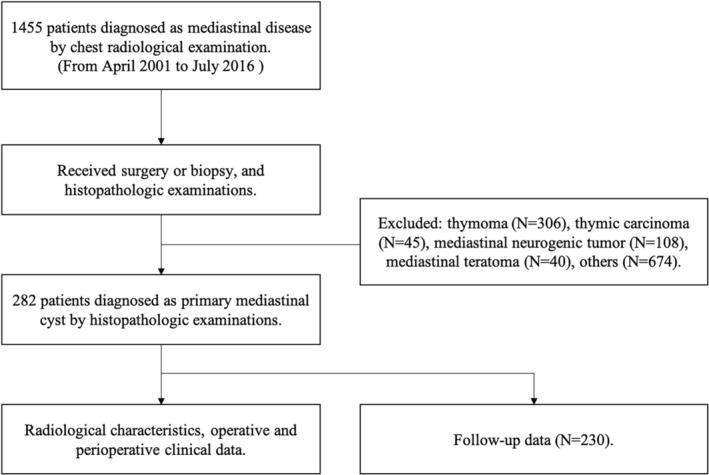
Methods: The medical records of all consecutive PMC patients, who underwent surgical resection from April 2001 to July 2016, were reviewed and 282 patients were included. Clinical characteristics, imaging features, and surgical outcomes were analyzed. Follow-up data were successfully obtained from 230 PMC patients by telephone or outpatient clinic annually. The latest follow-up was July 2019.
Results: VATS was performed in 278 patients and four patients were converted into thoracotomy. The mean operation time and intraoperative bleeding were 102.4 ± 40.9 minutes (range 25-360 minutes) and 52.4 ± 75.1 mL (range 5-600 mL), respectively. The intra- and postoperative complication rates were 2.8 and 5.7%, respectively. Seven patients with bronchogenic cysts showed severe cyst adhesion to vital mediastinal structures and thus had incomplete resection. Multivariable logistic analysis revealed that a maximal cyst diameter greater than 5 cm was significantly associated with increased risks of operation time extension (OR = 2.106; 95% CI: 1.147-3.865, P = 0.016) and intraoperative blood loss increase (OR = 4.428; 95% CI: 1.243-16.489, P = 0.022). A total of 230 patients had follow-up data. The median follow-up time was 70 months (range, 36-210 months). No local recurrence was observed.
Conclusions: Surgical resection by VATS may be recommended for PMC management as a primary therapeutic strategy. Cysts with a maximum diameter greater than 5 cm or cysts adjacent to vital mediastinal structures can increase the surgical difficulties.
Key points: • Significant findings of the study A diameter >5 cm and adhesions significantly increased the risk of operation time extension together with increased blood loss. • What this study adds Cysts with a diameter >5 cm or those adjacent to vital mediastinal structures increased the potential for surgical difficulties.
Keywords: Bronchogenic cyst; primary mediastinal cyst; thymic cyst; video-assisted thoracic surgery (VATS).
© 2020 The Authors. Thoracic Cancer published by China Lung Oncology Group and John Wiley & Sons Australia, Ltd.
Figures
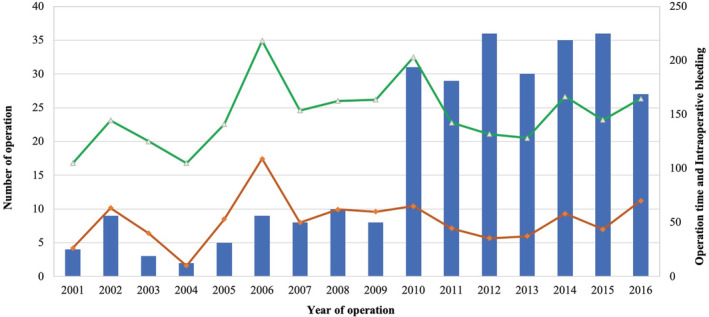
 ) Number of operation, (
) Number of operation, ( ) Intraoperative bleeding (mL), and (
) Intraoperative bleeding (mL), and ( ) Operation time (minutes).
) Operation time (minutes).
References
-
- Takeda S, Miyoshi S, Minami M, Ohta M, Masaoka A, Matsuda H. Clinical spectrum of mediastinal cysts. Chest 2003; 124: 125–32. - PubMed
-
- Kozu Y, Suzuki K, Oh S, Matsunaga T, Tsushima Y, Takamochi K. Single institutional experience with primary mediastinal cysts: Clinicopathological study of 108 resected cases. Ann Thorac Cardiovasc Surg 2014; 20: 365–9. - PubMed
-
- Kirmani B, Sogliani F. Should asymptomatic bronchogenic cysts in adults be treated conservatively or with surgery? Interact Cardiovasc Thorac Surg 2010; 11: 649–59. - PubMed
-
- Jeung MY, Gasser B, Gangi A. et al Imaging of cystic masses of the mediastinum. Radiographics 2002; 22 (suppl_1): S79–93. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
