

Retrospective Observational Study of Brain MRI Findings in Patients with Acute SARS-CoV-2 Infection and Neurologic Manifestations
- PMID: 32677875
- PMCID: PMC7370354
- DOI: 10.1148/radiol.2020202422
Retrospective Observational Study of Brain MRI Findings in Patients with Acute SARS-CoV-2 Infection and Neurologic Manifestations
Abstract
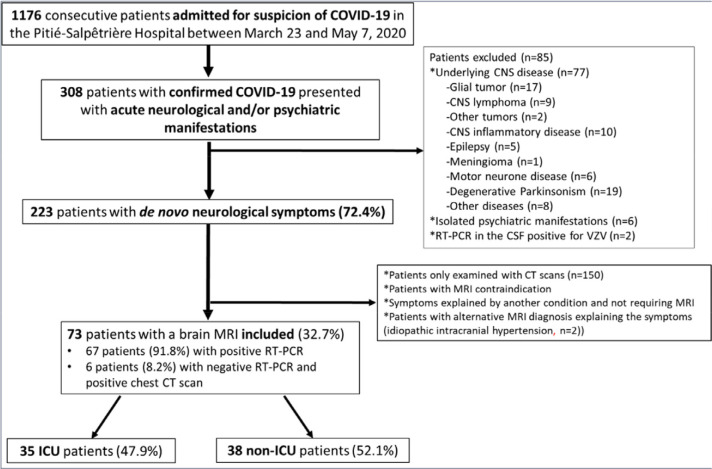
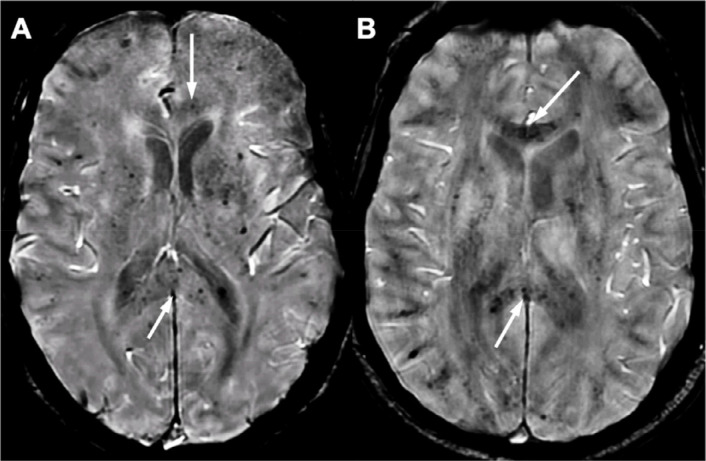
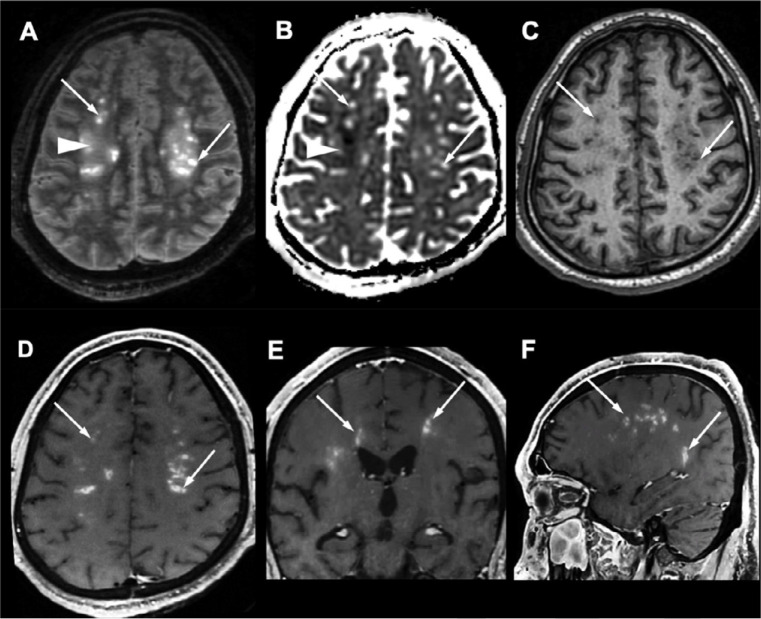
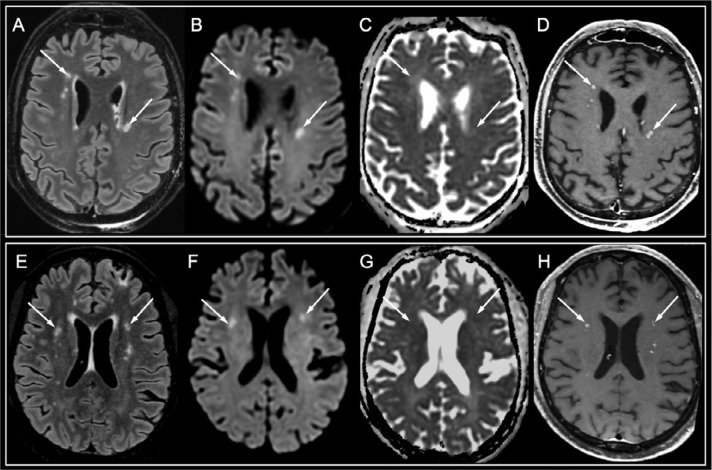
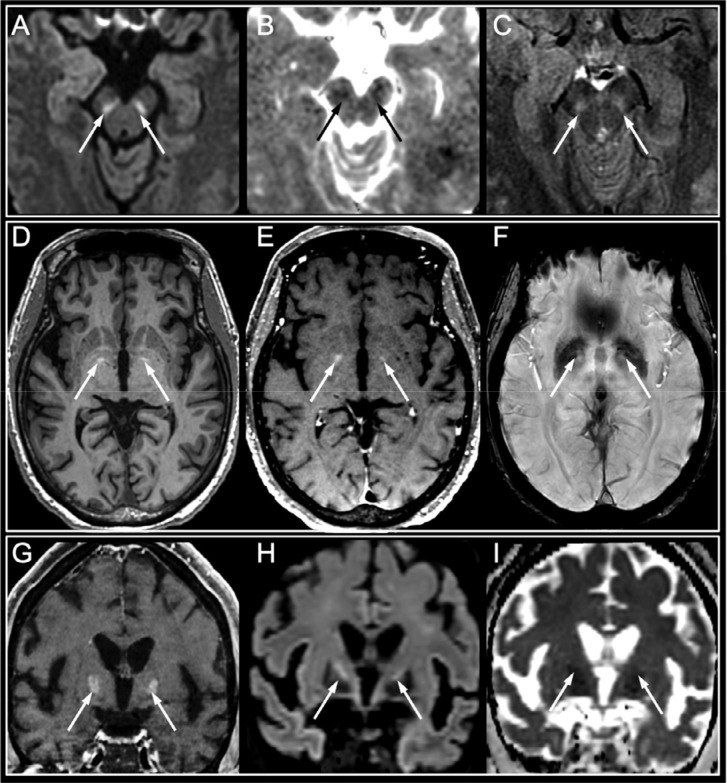
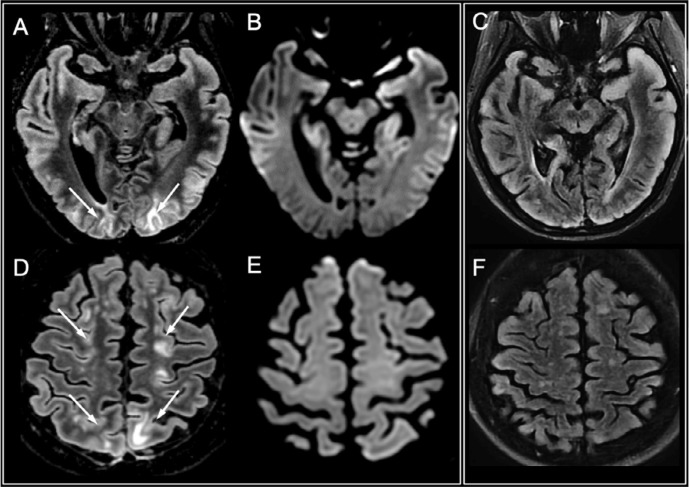
Background This study provides a detailed imaging assessment in a large series of patients infected with coronavirus disease 2019 (COVID-19) and presenting with neurologic manifestations. Purpose To review the MRI findings associated with acute neurologic manifestations in patients with COVID-19. Materials and Methods This was a cross-sectional study conducted between March 23 and May 7, 2020, at the Pitié-Salpêtrière Hospital, a reference center for COVID-19 in the Paris area. Adult patients were included if they had a diagnosis of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection with acute neurologic manifestations and referral for brain MRI. Patients with a prior history of neurologic disease were excluded. The characteristics and frequency of different MRI features were investigated. The findings were analyzed separately in patients in intensive care units (ICUs) and other departments (non-ICU). Results During the inclusion period, 1176 patients suspected of having COVID-19 were hospitalized. Of 308 patients with acute neurologic symptoms, 73 met the inclusion criteria and were included (23.7%): thirty-five patients were in the ICU (47.9%) and 38 were not (52.1%). The mean age was 58.5 years ± 15.6 [standard deviation], with a male predominance (65.8% vs 34.2%). Forty-three patients had abnormal MRI findings 2-4 weeks after symptom onset (58.9%), including 17 with acute ischemic infarct (23.3%), one with a deep venous thrombosis (1.4%), eight with multiple microhemorrhages (11.3%), 22 with perfusion abnormalities (47.7%), and three with restricted diffusion foci within the corpus callosum consistent with cytotoxic lesions of the corpus callosum (4.1%). Multifocal white matter-enhancing lesions were seen in four patients in the ICU (5%). Basal ganglia abnormalities were seen in four other patients (5%). Cerebrospinal fluid analyses were negative for SARS-CoV-2 in all patients tested (n = 39). Conclusion In addition to cerebrovascular lesions, perfusion abnormalities, cytotoxic lesions of the corpus callosum, and intensive care unit-related complications, we identified two patterns including white matter-enhancing lesions and basal ganglia abnormalities that could be related to severe acute respiratory syndrome coronavirus 2 infection. © RSNA, 2020 Online supplemental material is available for this article.
Figures
Similar articles
-
Brain MRI Findings in Severe COVID-19: A Retrospective Observational Study.Radiology. 2020 Nov;297(2):E242-E251. doi: 10.1148/radiol.2020202222. Epub 2020 Jun 16. Radiology. 2020. PMID: 32544034 Free PMC article.
-
Nervous System Involvement in Coronavirus Disease 2019: Results from a Retrospective Consecutive Neuroimaging Cohort.Radiology. 2020 Dec;297(3):E324-E334. doi: 10.1148/radiol.2020202791. Epub 2020 Jul 30. Radiology. 2020. PMID: 32729812 Free PMC article.
-
Coronavirus 2019 (COVID-19)-Associated Encephalopathies and Cerebrovascular Disease: The New Orleans Experience.World Neurosurg. 2020 Sep;141:e437-e446. doi: 10.1016/j.wneu.2020.05.192. Epub 2020 May 28. World Neurosurg. 2020. PMID: 32474092 Free PMC article.
-
Brain abnormalities in COVID-19 acute/subacute phase: A rapid systematic review.Brain Behav Immun. 2020 Oct;89:543-554. doi: 10.1016/j.bbi.2020.07.014. Epub 2020 Jul 17. Brain Behav Immun. 2020. PMID: 32682993 Free PMC article.
-
Neurovascular and perfusion imaging findings in coronavirus disease 2019: Case report and literature review.Neuroradiol J. 2020 Oct;33(5):368-373. doi: 10.1177/1971400920941652. Epub 2020 Jul 15. Neuroradiol J. 2020. PMID: 32666873 Free PMC article. Review.
Cited by
-
Association of Clinical, Biological, and Brain Magnetic Resonance Imaging Findings With Electroencephalographic Findings for Patients With COVID-19.JAMA Netw Open. 2021 Mar 1;4(3):e211489. doi: 10.1001/jamanetworkopen.2021.1489. JAMA Netw Open. 2021. PMID: 33720371 Free PMC article.
-
Brutal neurological disorder after SARS-CoV-2 infection.Rev Med Interne. 2022 Jun;43(6):385-386. doi: 10.1016/j.revmed.2022.01.008. Epub 2022 Feb 3. Rev Med Interne. 2022. PMID: 36852932 Free PMC article. No abstract available.
-
Transient splenial lesions of the corpus callosum and infectious diseases.Acute Crit Care. 2022 Aug;37(3):269-275. doi: 10.4266/acc.2022.00864. Epub 2022 Aug 17. Acute Crit Care. 2022. PMID: 35977887 Free PMC article.
-
Modulating neuroinflammation in COVID-19 patients with obsessive-compulsive disorder.J Psychiatr Res. 2022 May;149:367-373. doi: 10.1016/j.jpsychires.2021.11.025. Epub 2021 Nov 17. J Psychiatr Res. 2022. PMID: 34809994 Free PMC article. Review.
-
Brain MRI findings in neurologically symptomatic COVID-19 patients: a systematic review and meta-analysis.J Neurol. 2023 Nov;270(11):5131-5154. doi: 10.1007/s00415-023-11914-9. Epub 2023 Aug 3. J Neurol. 2023. PMID: 37535100 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
