

Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19
- PMID: 32678428
- PMCID: PMC7483437
- DOI: 10.1182/blood.2020007252
Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19
Abstract
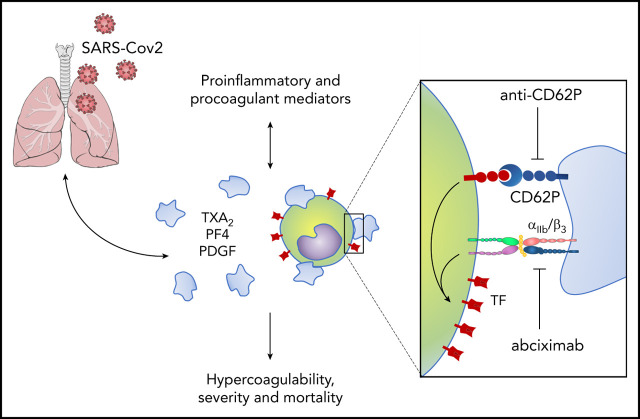
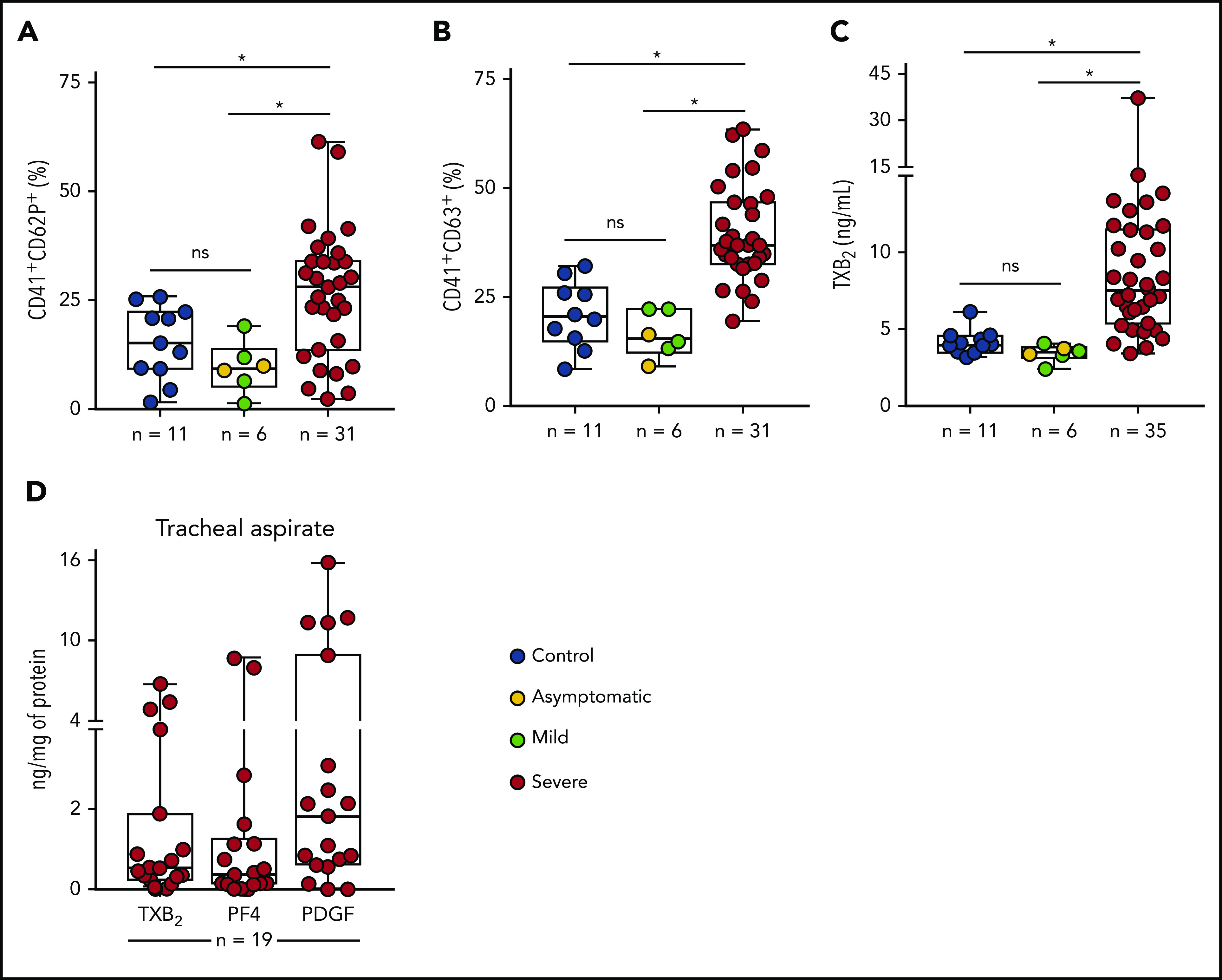
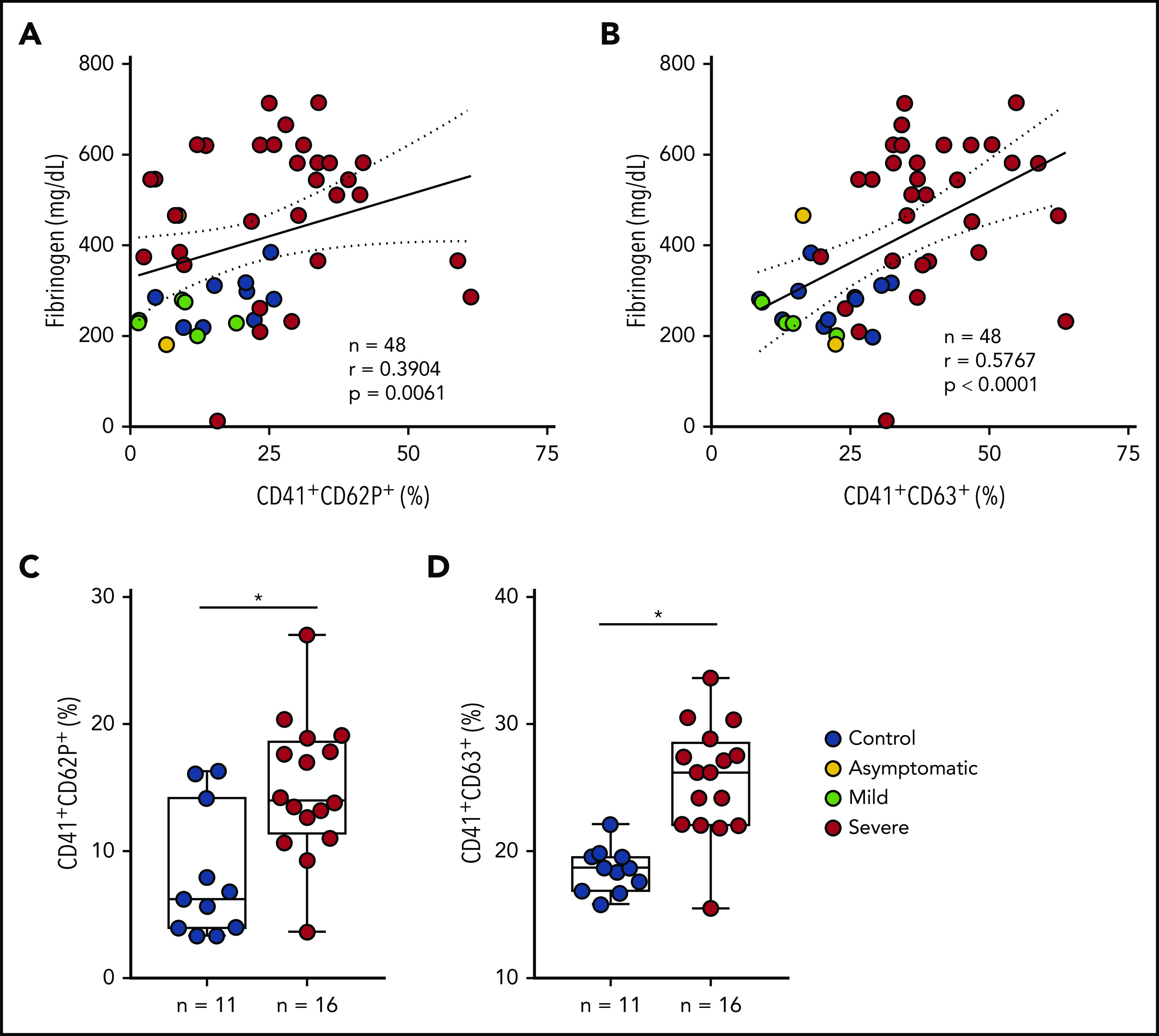
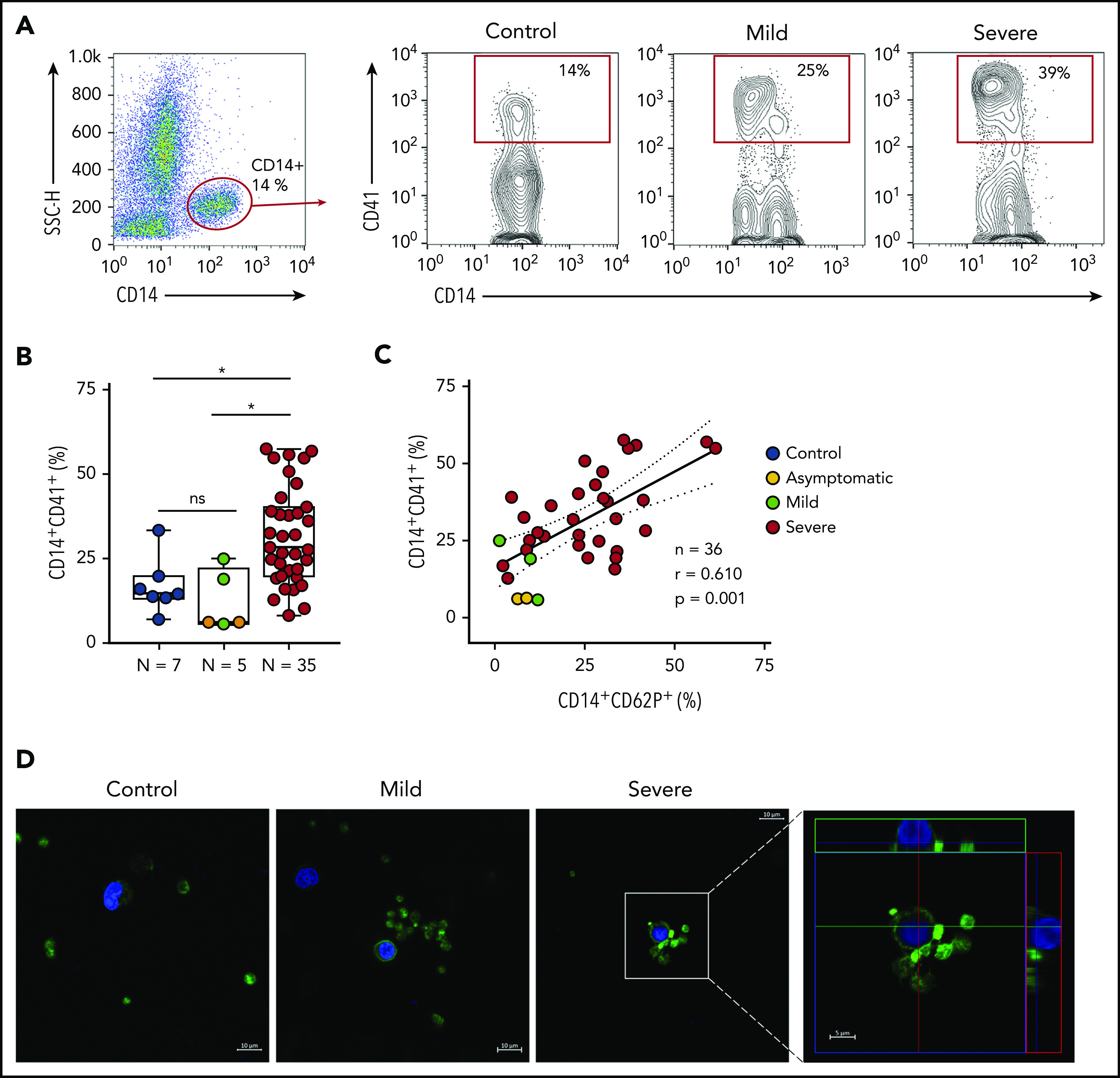
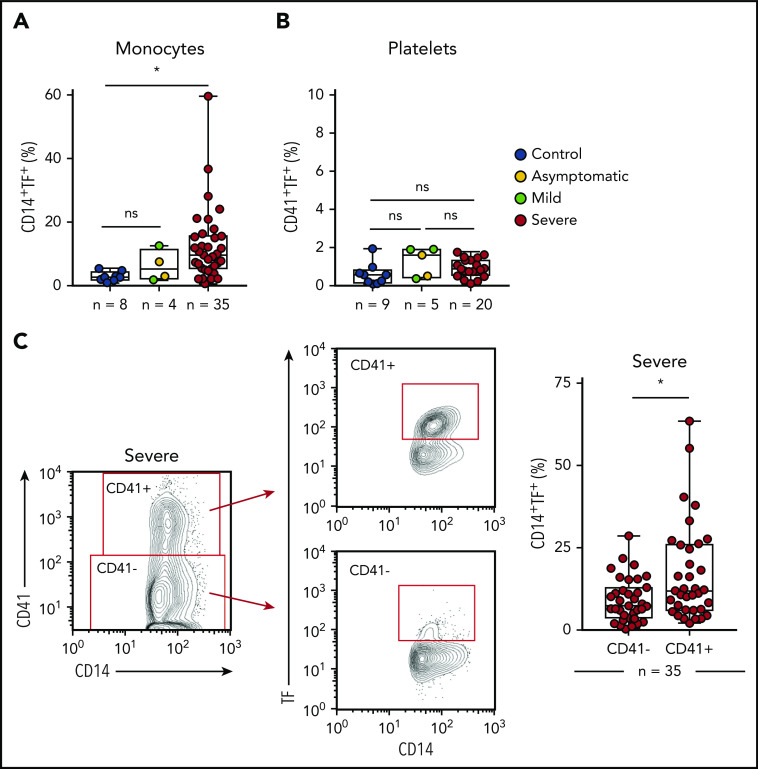
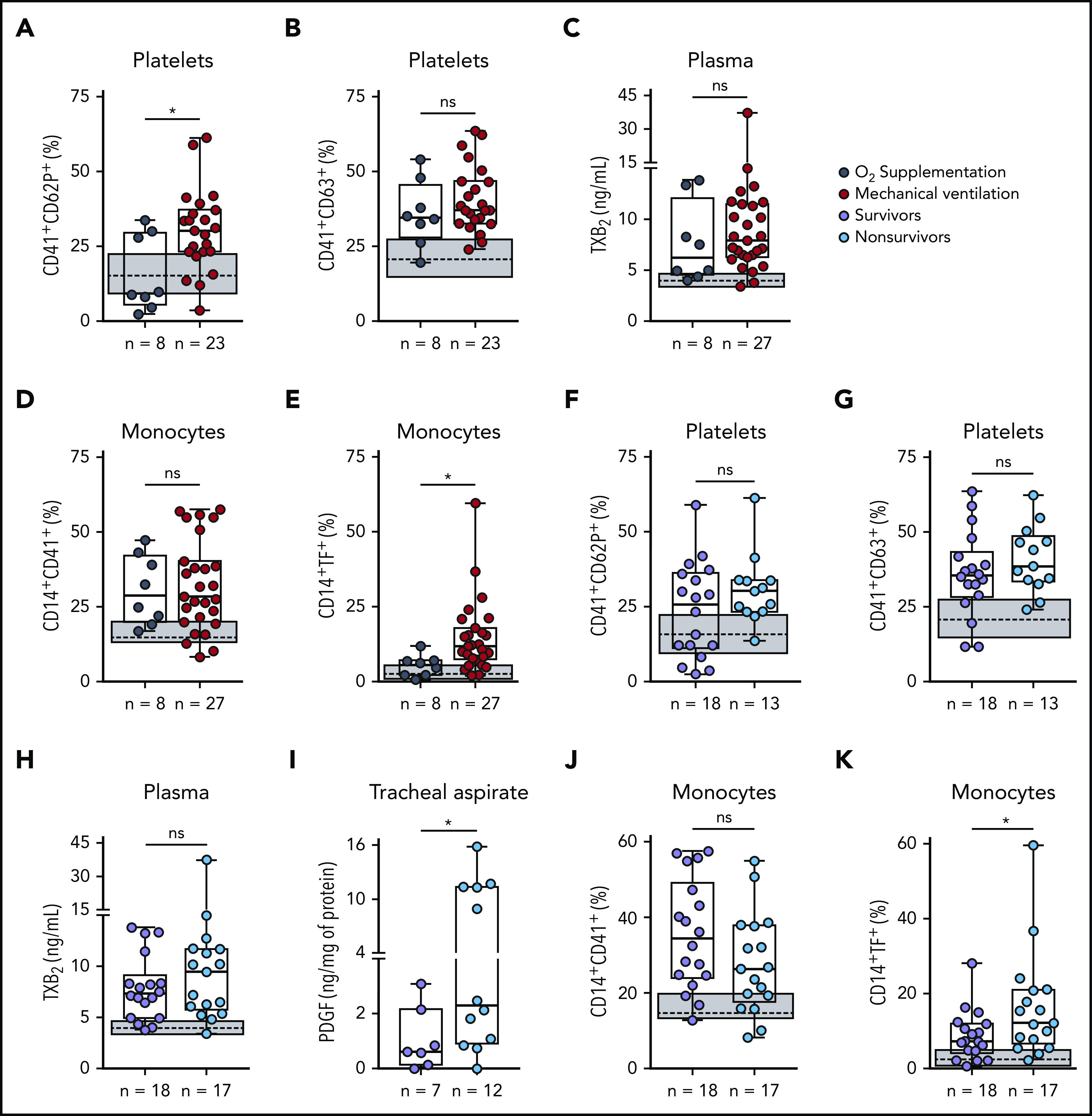
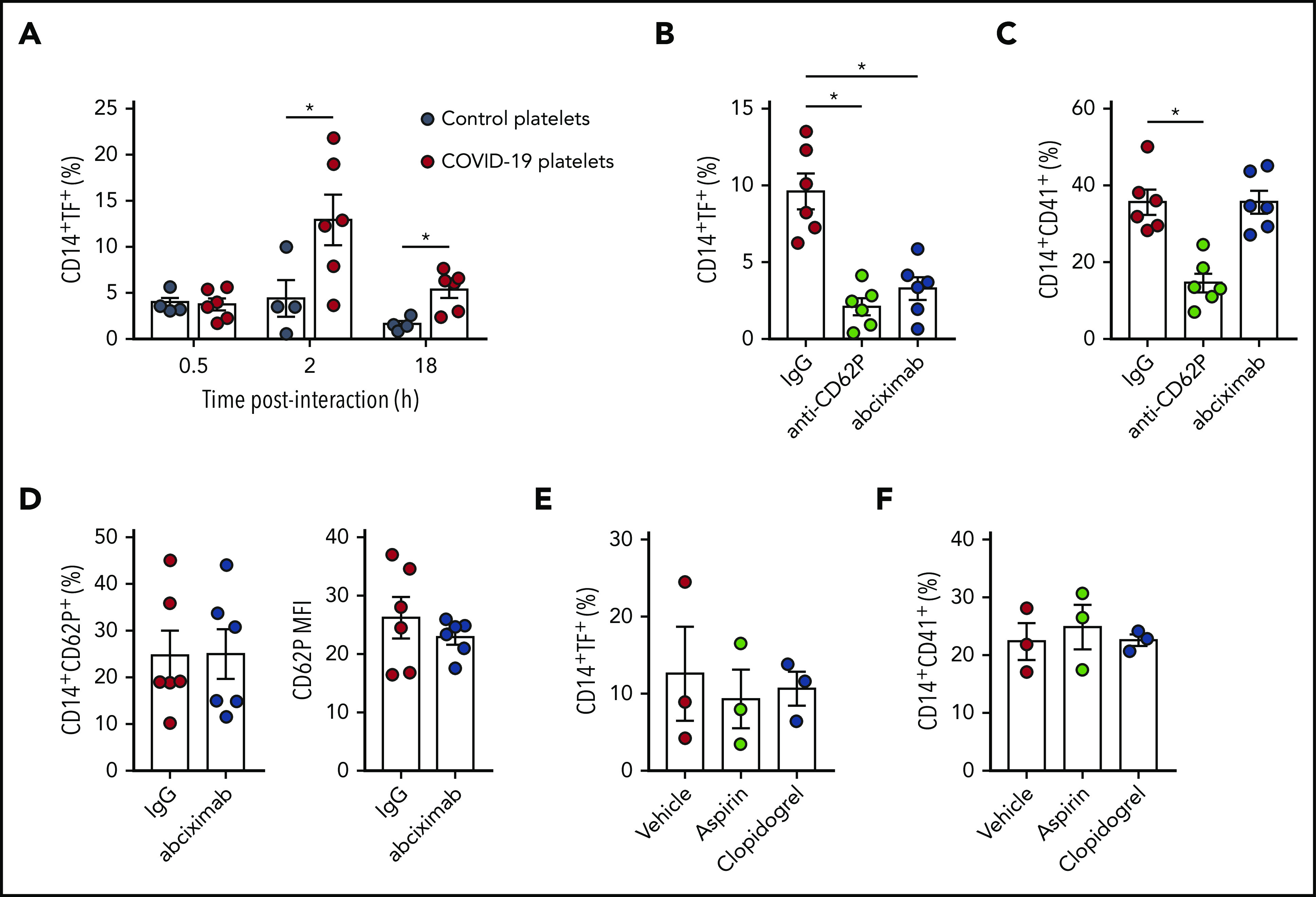
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is an emergent pathogen responsible for the coronavirus disease 2019 (COVID-19). Since its emergence, the novel coronavirus has rapidly achieved pandemic proportions causing remarkably increased morbidity and mortality around the world. A hypercoagulability state has been reported as a major pathologic event in COVID-19, and thromboembolic complications listed among life-threatening complications of the disease. Platelets are chief effector cells of hemostasis and pathological thrombosis. However, the participation of platelets in the pathogenesis of COVID-19 remains elusive. This report demonstrates that increased platelet activation and platelet-monocyte aggregate formation are observed in severe COVID-19 patients, but not in patients presenting mild COVID-19 syndrome. In addition, exposure to plasma from severe COVID-19 patients increased the activation of control platelets ex vivo. In our cohort of COVID-19 patients admitted to the intensive care unit, platelet-monocyte interaction was strongly associated with tissue factor (TF) expression by the monocytes. Platelet activation and monocyte TF expression were associated with markers of coagulation exacerbation as fibrinogen and D-dimers, and were increased in patients requiring invasive mechanical ventilation or patients who evolved with in-hospital mortality. Finally, platelets from severe COVID-19 patients were able to induce TF expression ex vivo in monocytes from healthy volunteers, a phenomenon that was inhibited by platelet P-selectin neutralization or integrin αIIb/β3 blocking with the aggregation inhibitor abciximab. Altogether, these data shed light on new pathological mechanisms involving platelet activation and platelet-dependent monocyte TF expression, which were associated with COVID-19 severity and mortality.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
Comment in
-
COVID-19 concerns aggregate around platelets.Blood. 2020 Sep 10;136(11):1221-1223. doi: 10.1182/blood.2020007805. Blood. 2020. PMID: 32957116 Free PMC article.
-
ART and science of keeping HIV out of the blood supply.Blood. 2020 Sep 10;136(11):1223-1224. doi: 10.1182/blood.2020008122. Blood. 2020. PMID: 32957118 No abstract available.
References
-
- World Health Organization Coronavirus Disease (COVID-19) Situation Report-122. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... Accessed 22 May 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
