

Rapid implementation of SARS-CoV-2 sequencing to investigate cases of health-care associated COVID-19: a prospective genomic surveillance study
- PMID: 32679081
- PMCID: PMC7806511
- DOI: 10.1016/S1473-3099(20)30562-4
Rapid implementation of SARS-CoV-2 sequencing to investigate cases of health-care associated COVID-19: a prospective genomic surveillance study
Erratum in
-
Correction to Lancet Infect Dis 2020; 20: 1263-72.Lancet Infect Dis. 2021 Mar;21(3):e36. doi: 10.1016/S1473-3099(21)00046-3. Epub 2021 Jan 22. Lancet Infect Dis. 2021. PMID: 33493442 Free PMC article. No abstract available.
-
Correction to Lancet Infect Dis 2020; 20: 1263-72.Lancet Infect Dis. 2021 Mar;21(3):e36. doi: 10.1016/S1473-3099(21)00089-X. Epub 2021 Feb 11. Lancet Infect Dis. 2021. PMID: 33581747 Free PMC article. No abstract available.
Abstract
Background: The burden and influence of health-care associated severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections is unknown. We aimed to examine the use of rapid SARS-CoV-2 sequencing combined with detailed epidemiological analysis to investigate health-care associated SARS-CoV-2 infections and inform infection control measures.
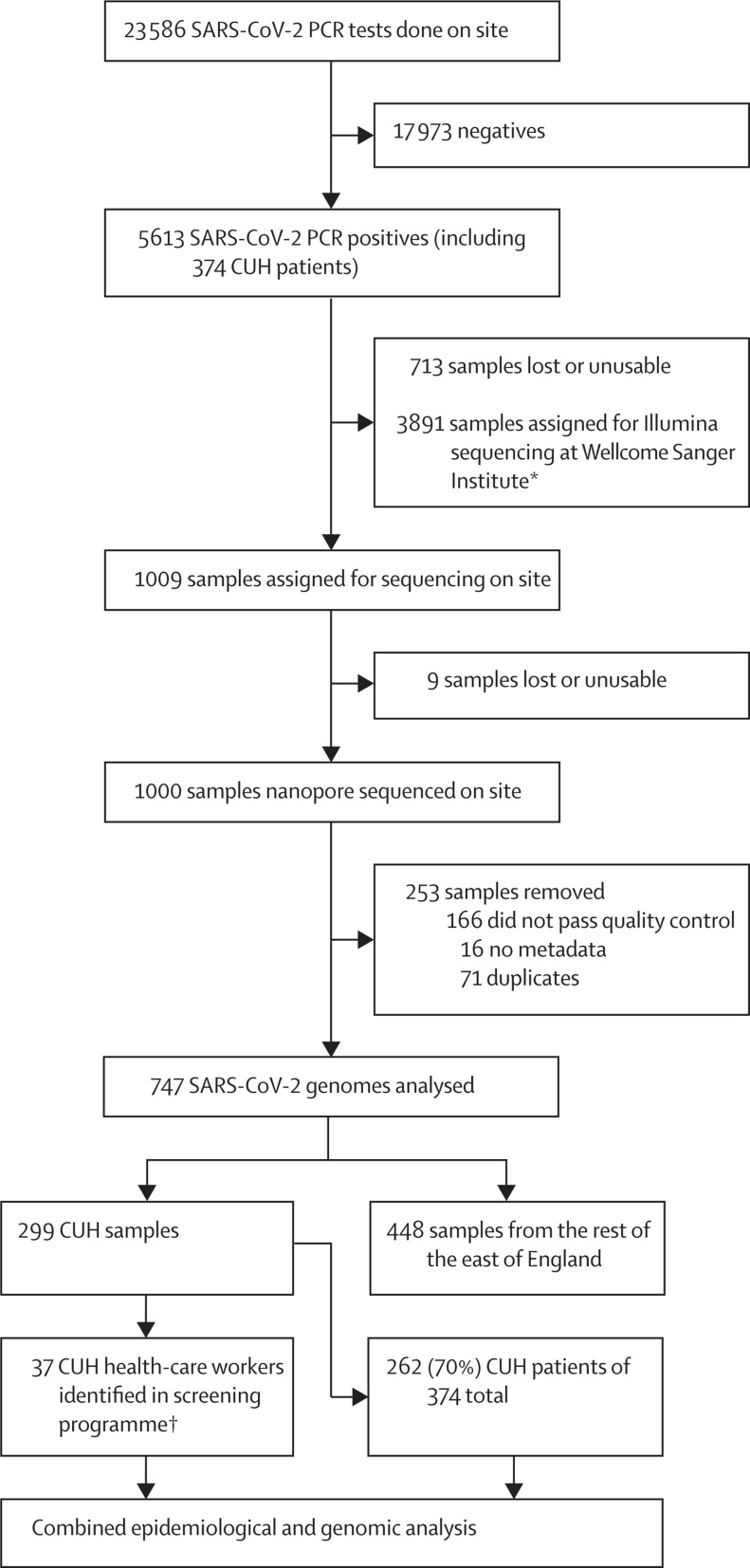
Methods: In this prospective surveillance study, we set up rapid SARS-CoV-2 nanopore sequencing from PCR-positive diagnostic samples collected from our hospital (Cambridge, UK) and a random selection from hospitals in the East of England, enabling sample-to-sequence in less than 24 h. We established a weekly review and reporting system with integration of genomic and epidemiological data to investigate suspected health-care associated COVID-19 cases.
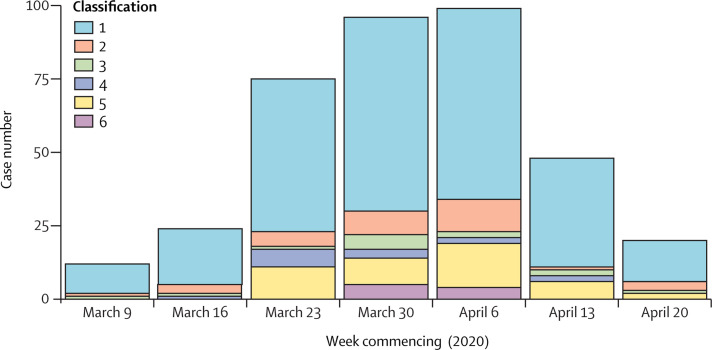
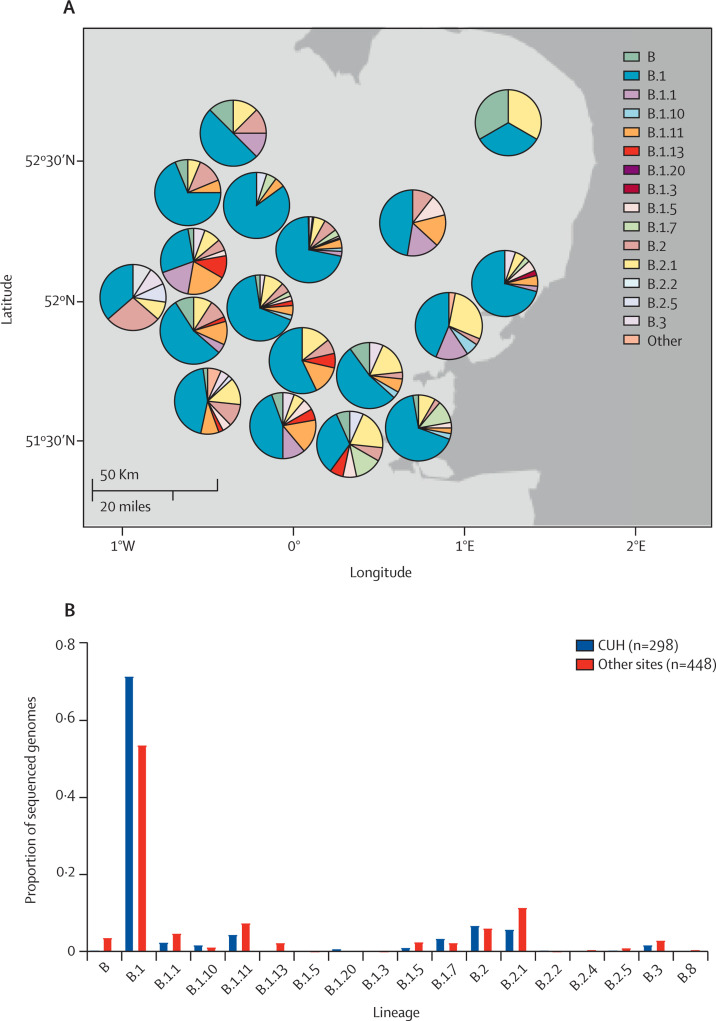
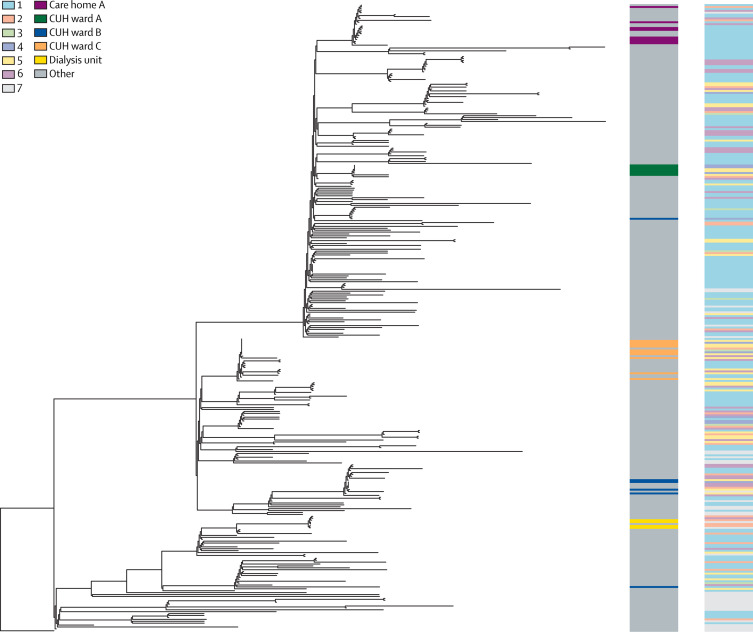
Findings: Between March 13 and April 24, 2020, we collected clinical data and samples from 5613 patients with COVID-19 from across the East of England. We sequenced 1000 samples producing 747 high-quality genomes. We combined epidemiological and genomic analysis of the 299 patients from our hospital and identified 35 clusters of identical viruses involving 159 patients. 92 (58%) of 159 patients had strong epidemiological links and 32 (20%) patients had plausible epidemiological links. These results were fed back to clinical, infection control, and hospital management teams, leading to infection-control interventions and informing patient safety reporting.
Interpretation: We established real-time genomic surveillance of SARS-CoV-2 in a UK hospital and showed the benefit of combined genomic and epidemiological analysis for the investigation of health-care associated COVID-19. This approach enabled us to detect cryptic transmission events and identify opportunities to target infection-control interventions to further reduce health-care associated infections. Our findings have important implications for national public health policy as they enable rapid tracking and investigation of infections in hospital and community settings.
Funding: COVID-19 Genomics UK funded by the Department of Health and Social Care, UK Research and Innovation, and the Wellcome Sanger Institute.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
COVID-19: from rapid genome sequencing to fast decisions.Lancet Infect Dis. 2020 Nov;20(11):1218. doi: 10.1016/S1473-3099(20)30580-6. Epub 2020 Jul 14. Lancet Infect Dis. 2020. PMID: 32679087 Free PMC article. No abstract available.
-
Applying prospective genomic surveillance to support investigation of hospital-onset COVID-19.Lancet Infect Dis. 2021 Jul;21(7):916-917. doi: 10.1016/S1473-3099(21)00251-6. Epub 2021 May 10. Lancet Infect Dis. 2021. PMID: 33984262 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
