

Nephroprotection by SGLT2 Inhibition: Back to the Future?
- PMID: 32679744
- PMCID: PMC7408701
- DOI: 10.3390/jcm9072243
Nephroprotection by SGLT2 Inhibition: Back to the Future?
Abstract
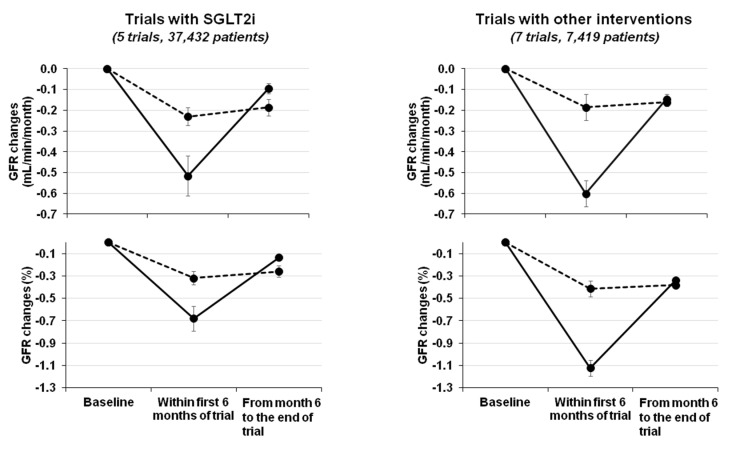
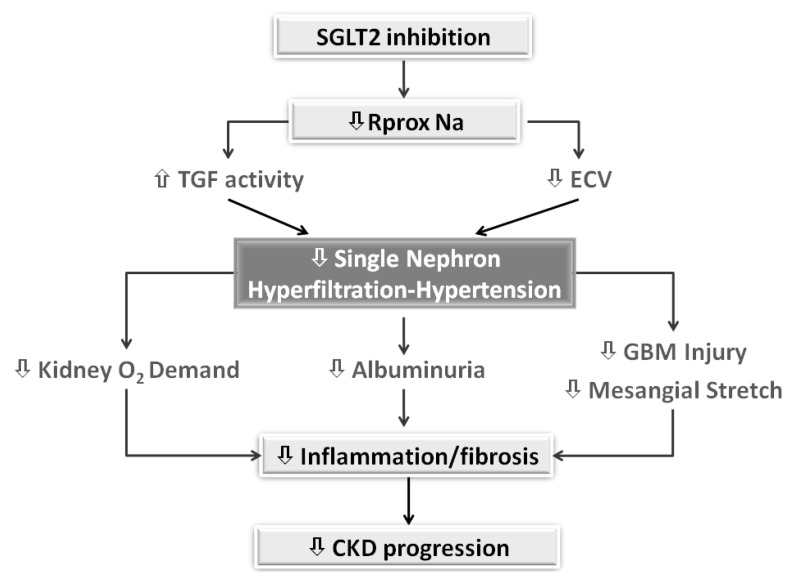
The introduction of sodium/glucose cotransporter 2 inhibitors (SGLT2i) has opened new perspectives for the management of diabetic population at risk of or with chronic kidney disease (CKD). More important, recent, large real-world studies have repositioned the nephroprotective efficacy of SGLT2i emerged from randomized trials within the frame of effectiveness. Furthermore, the salutary effects of these agents may extend to the nondiabetic population according to the positive results of current studies. Nevertheless, the clear benefits of these agents on the prevention of organ damage contrast with their unexpected, limited use in clinical practice. One potential barrier is the acute decline in glomerular filtration rate (GFR) commonly observed at the beginning of treatment. This phenomenon is reminiscent of the early response to the traditional nephroprotective interventions, namely blood pressure lowering, dietary protein and salt restriction and the inhibition of the renin-angiotensin system. Under this perspective, the "check-mark" sign observed in the GFR trajectory over the first weeks of SGT2i therapy should renew interest on the very basic goal of CKD treatment, i.e., alleviate hyperfiltration in viable nephrons in order to prolong their function.
Keywords: SGLT2-inhibition; chronic kidney disease; nephroprotection.
Conflict of interest statement
L.D.N. has received fees for scientific consultation and/or lectures from Astellas, AstraZeneca, Mundibiopharma and Vifor Pharma. R.M. was a member of advisory boards for Astellas and an invited speaker at meetings supported by Amgen and Vifor Pharma. F.G., G.C and C.G. do not have any conflict of interest to declare.
Figures
References
-
- Lundström U.H., Gasparini A., Bellocco R., Qureshi A.R., Carrero J.-J., Evans M. Low renal replacement therapy incidence among slowly progressing elderly chronic kidney disease patients referred to nephrology care: An observational study. BMC Nephrol. 2017;18:59. doi: 10.1186/s12882-017-0473-1. - DOI - PMC - PubMed
-
- Brück K., Jager K.J., Zoccali C., Bello A.K., Minutolo R., Ioannou K., Verbeke F., Völzke H., Ärnlöv J., Leonardis D., et al. Different rates of progression and mortality in patients with chronic kidney disease at outpatient nephrology clinics across Europe. Kidney Int. 2018;93:1432–1441. doi: 10.1016/j.kint.2018.01.008. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
