

Locoregional Therapy Approaches for Hepatocellular Carcinoma: Recent Advances and Management Strategies
- PMID: 32679897
- PMCID: PMC7409274
- DOI: 10.3390/cancers12071914
Locoregional Therapy Approaches for Hepatocellular Carcinoma: Recent Advances and Management Strategies
Abstract
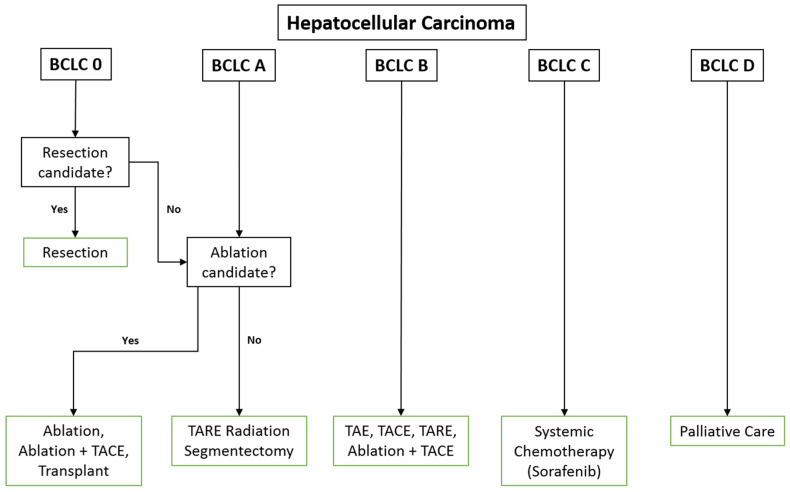
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and third leading cause of cancer-related mortality worldwide. While surgical resection and transplantation are the standard first-line treatments for early-stage HCC, most patients do not fulfill criteria for surgery. Fortunately, catheter-directed and percutaneous locoregional approaches have evolved as major treatment modalities for unresectable HCC. Improved outcomes have been achieved with novel techniques which can be employed for diverse applications ranging from curative-intent for small localized tumors, to downstaging or bridging to resection and transplantation for early and intermediate disease, and locoregional control and palliation for advanced disease. This review explores recent advances in liver-directed techniques for HCC including bland transarterial embolization, chemoembolization, radioembolization, and ablative therapies, with a focus on patient selection, procedural technique, periprocedural management, and outcomes.
Keywords: SIRT; TACE; TAE; TARE; ablation; chemoembolization; hepatocellular carcinoma; immunotherapy; radioembolization; transarterial embolization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Howlader N., Noone A.M., Krapcho M., Miller D., Brest A., Yu M., Ruhl J., Tatalovich Z., Mariotto A., Lewis D.R., et al., editors. EEER Cancer Statistics Review, 1975–2016. National Cancer Institute; Bethesda, MD, USA: 2018. [(accessed on 1 July 2020)]. Available online: https://seer.cancer.gov/csr/1975_2016/
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
