

Global activation of oncogenic pathways underlies therapy resistance in diffuse midline glioma
- PMID: 32680567
- PMCID: PMC7367358
- DOI: 10.1186/s40478-020-00992-9
Global activation of oncogenic pathways underlies therapy resistance in diffuse midline glioma
Abstract
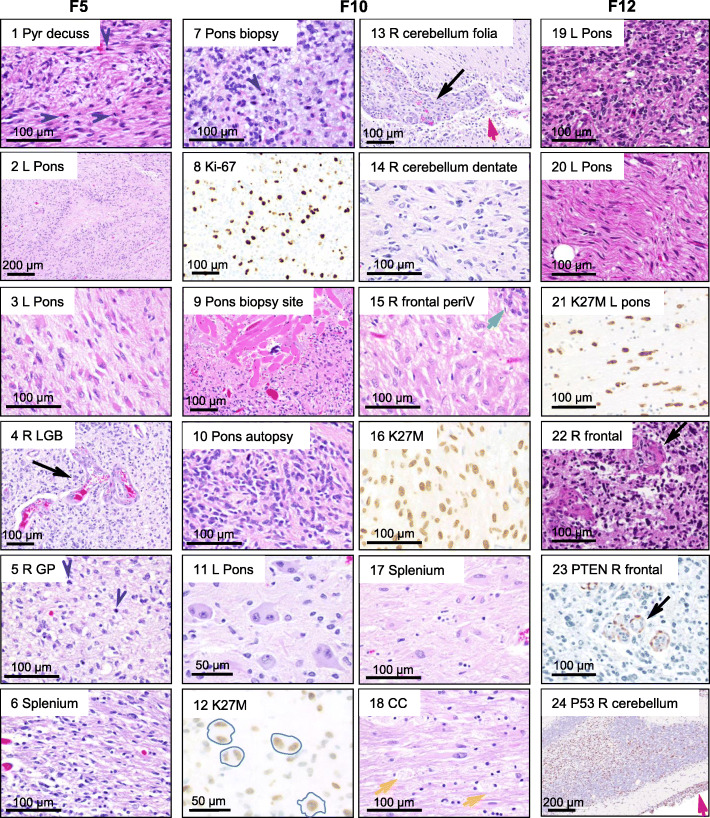
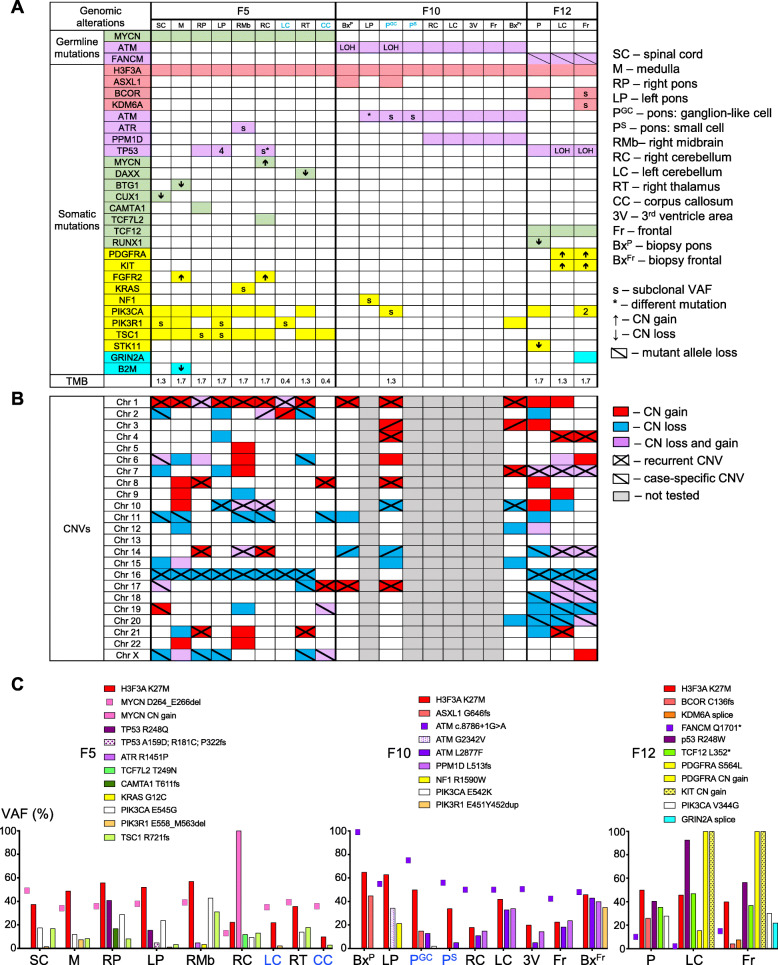
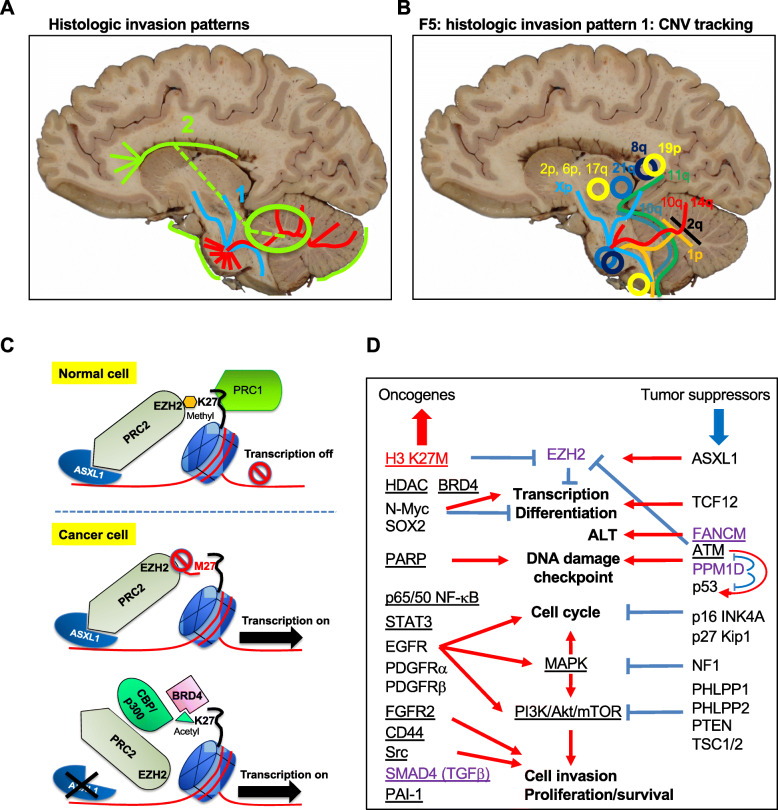
Diffuse midline gliomas (DMGs) are aggressive pediatric brain tumors with dismal prognosis due to therapy-resistant tumor growth and invasion. We performed the first integrated histologic/genomic/proteomic analysis of 21 foci from three pontine DMG cases with supratentorial dissemination. Histone H3.3-K27M was the driver mutation, usually at high variant allele fraction due to recurrent chromosome 1q copy number gain, in combination with germline variants in ATM, FANCM and MYCN genes. Both previously reported and novel recurrent copy number variations and somatic pathogenic mutations in chromatin remodeling, DNA damage response and PI3K/MAPK growth pathways were variably detected, either in multiple or isolated foci. Proteomic analysis showed global upregulation of histone H3, lack of H3-K27 trimethylation, and further impairment of polycomb repressive complex 2 by ASXL1 downregulation. Activation of oncogenic pathways resulted from combined upregulation of N-MYC, SOX2, p65/p50 NF-κB and STAT3 transcription factors, EGFR, FGFR2, PDGFRα/β receptor tyrosine kinases, and downregulation of PHLPP1/2, PTEN and p16/INK4A tumor suppressors. Upregulation of SMAD4, PAI-1, CD44, and c-SRC in multiple foci most likely contributed to invasiveness. This integrated comprehensive analysis revealed a complex spatiotemporal evolution in diffuse intrisic pontine glioma, recommending pontine and cerebellar biopsies for accurate populational genetic characterization, and delineated common signaling pathways and potential therapeutic targets. It also revealed an unsuspected activation of a multitude of oncogenic pathways, including cancer cell reprogramming, explaining the resistance of DMG to current therapies.
Keywords: Diffuse midline glioma, Autopsy, Next generation sequencing (NGS), Copy number variation (CNV), Proteomics.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Louis DN, Ohgaki H, Wiestler OD, Caveneee WK. WHO classification of Tumors of the central nervous system. Lyon: IARC; 2016. - PubMed
-
- Chiang JC, Ellison DW. Molecular pathology of paediatric central nervous system tumours. J Pathol. 2017;241:159–172. - PubMed
-
- Benitez-Ribas D, Cabezon R, Florez-Grau G, Molero MC, Puerta P, Guillen A, et al. Immune response generated with the Administration of Autologous Dendritic Cells Pulsed with an Allogenic Tumoral cell-lines lysate in patients with newly diagnosed diffuse intrinsic Pontine Glioma. Front Oncol. 2018;8:127. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
