

Custom total knee arthroplasty facilitates restoration of constitutional coronal alignment
- PMID: 32681286
- PMCID: PMC8866384
- DOI: 10.1007/s00167-020-06153-8
Custom total knee arthroplasty facilitates restoration of constitutional coronal alignment
Erratum in
-
Correction to: Custom total knee arthroplasty facilitates restoration of constitutional coronal alignment.Knee Surg Sports Traumatol Arthrosc. 2022 Feb;30(2):476. doi: 10.1007/s00167-020-06238-4. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 32860522 Free PMC article. No abstract available.
Abstract
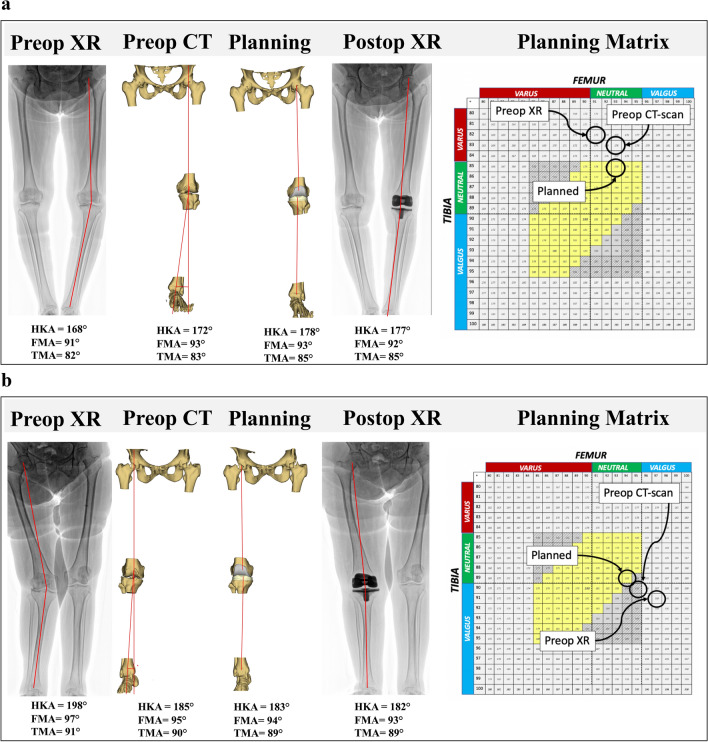
Purpose: To describe a strategy for coronal alignment using a computed tomography (CT) based custom total knee arthroplasty (TKA) system, and to evaluate the agreement between the planned and postoperative Hip-Knee-Ankle (HKA) angle, Femoral Mechanical Angle (FMA) and Tibial Mechanical Angle (TMA).
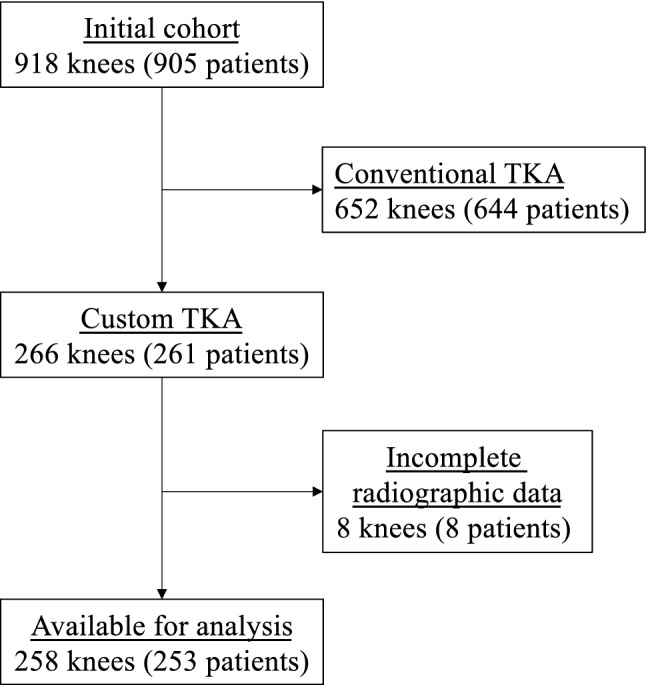
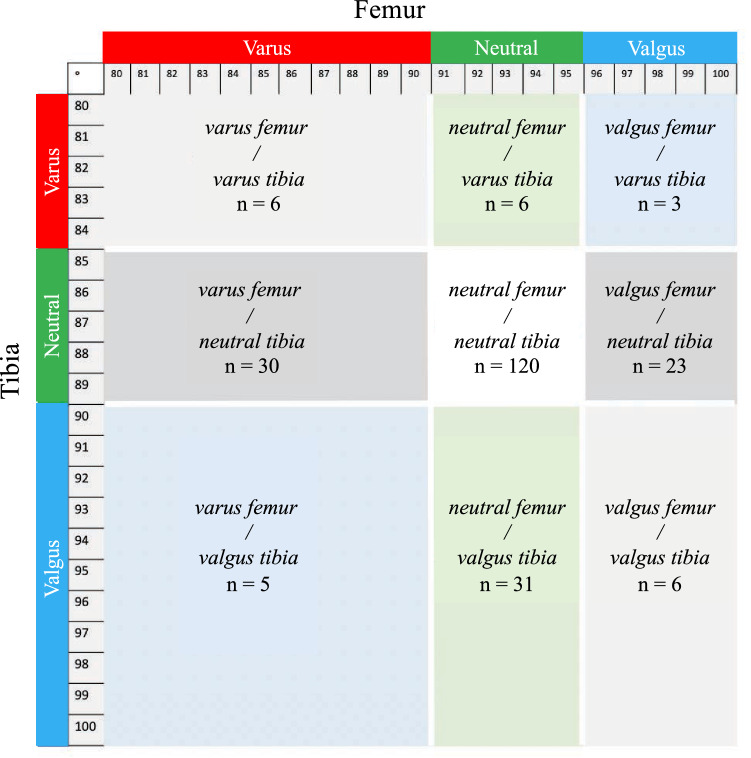
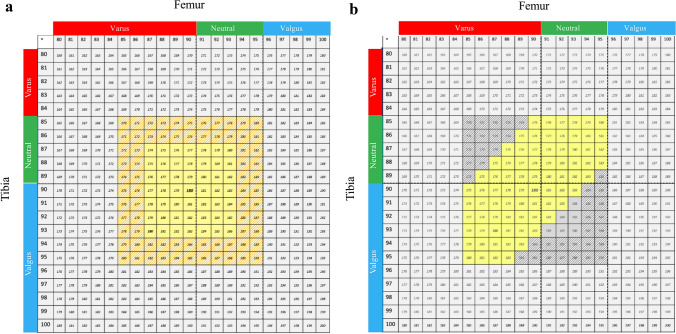
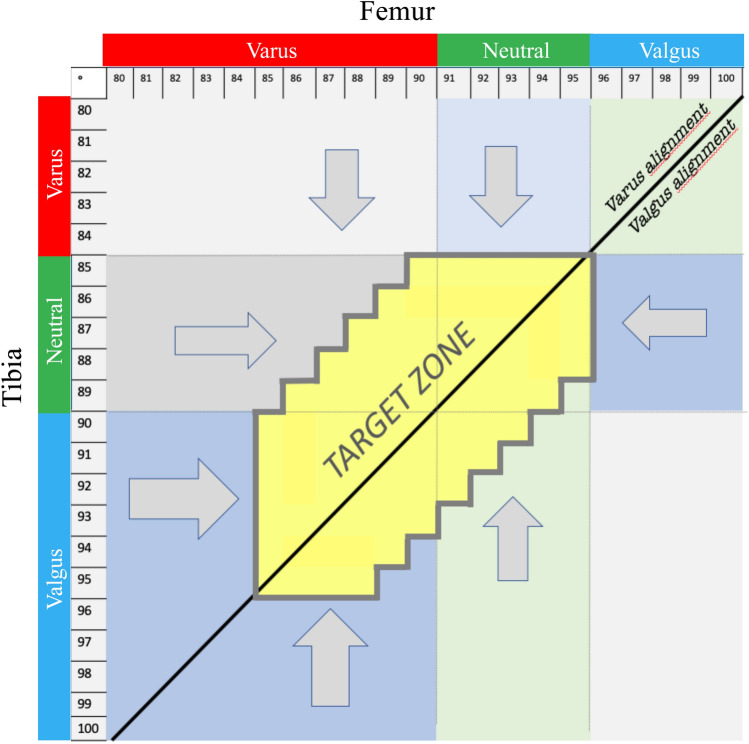
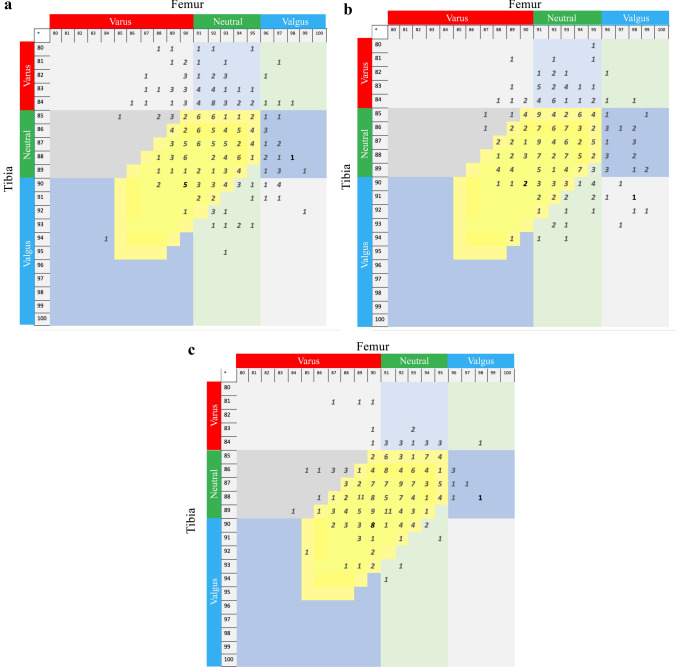
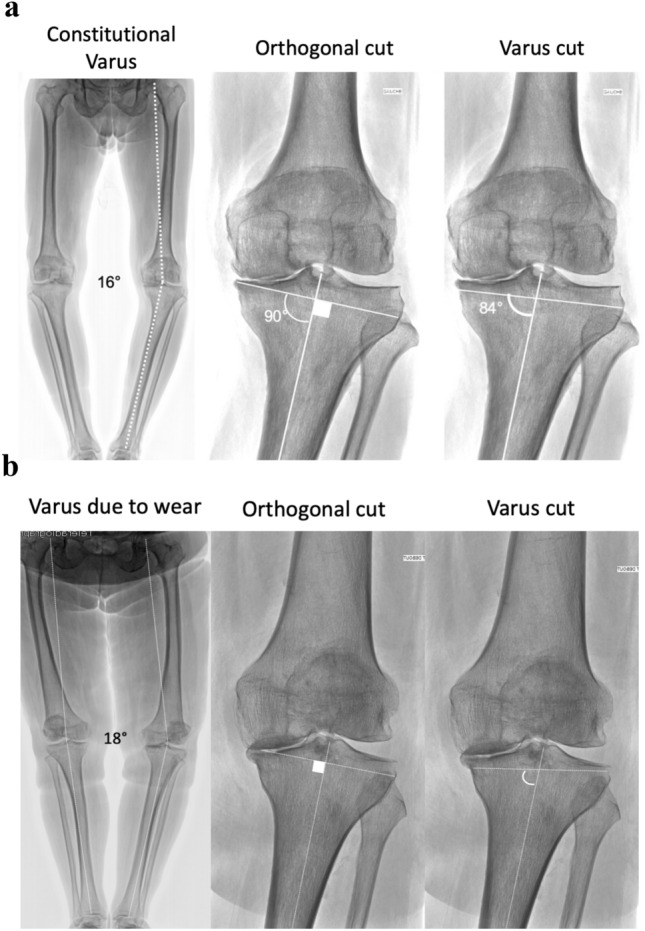
Methods: From a consecutive series of 918 primary TKAs, 266 (29%) knees received CT-based posterior-stabilized cemented custom TKA. In addition to a preoperative CT-scan, pre- and post-operative radiographs of weight-bearing long leg, anterior-posterior and lateral views of the knee were obtained, on which the FMA, TMA and HKA angles were measured. CT-based three-dimensional (3D) models enabled to correct for cases with bony wear by referring to the non-worn areas and to estimate the native pre-arthritic angles. The alignment technique aimed to preserve or restore constitutional alignment (CA) within predetermined limits, by defining a 'target zone' based on three criteria: 1) a ± 3° (range 87°-93°) primary tolerance for the femoral and tibial resections; 2) a ± 2° secondary tolerance for component obliquity, extending the bounds for FMA and TMA (range 85°-95°); 3) a planned HKA angle range of 175°-183°. Agreement between preoperative, planned and postoperative measurements of FMA, TMA and HKA angle were calculated using intra-class correlation coefficients (ICC).
Results: Preoperative radiograph and CT-scan measurements revealed that, respectively, 73 (28%) and 103 (40%) knees were in the 'target zone', whereas postoperative radiographs revealed that 217 (84%) TKAs were in the 'target zone'. Deviation from the planned angles were - 0.5° ± 1.8° for FMA, - 0.5° ± 1.8° for TMA, and - 1.1° ± 2.1° for HKA angle. Finally, the agreement between the planned and achieved targets, indicated by ICC, were good for FMA (0.701), fair for TMA (0.462) and fair for HKA angle (0.472).
Conclusion: Using this strategy for coronal alignment, 84% of custom TKAs were within the 'target zone' for FMA, TMA and HKA angles. These findings support the concepts of emerging personalized medicine technologies, and emphasise the importance of accurate strategies for preoperative planning, which are key to achieving satisfactory 'personalised alignment' that can further be improved by customisation of implant components.
Level of evidence: IV.
Keywords: Coronal alignment; Custom TKA; FMA; HKA; Patient-specific; TMA; Total knee arthroplasty; Total knee replacement.
© 2020. The Author(s).
Conflict of interest statement
MPB reports personal fees from DePuy Synthes, Wright Medical, Integra and Symbios. LB has nothing to declare. AL has nothing to declare. JC has nothing to declare. JHM has nothing to declare. COT reports personal fees from Symbios and Smith & Nephew. TASS reports personal fees from DePuy-Synthes and from Symbios.
Figures
References
-
- Abdel MP, Ollivier M, Parratte S, Trousdale RT, Berry DJ, Pagnano MW. Effect of postoperative mechanical axis alignment on survival and functional outcomes of modern total knee arthroplasties with cement: a concise follow-up at 20 years. J Bone Joint Surg Am. 2018;100(6):472–478. - PubMed
-
- Arbab D, Reimann P, Brucker M, Bouillon B, Luring C. Alignment in total knee arthroplasty—A comparison of patient-specific implants with the conventional technique. Knee. 2018;25(5):882–887. - PubMed
-
- Berger RA, Crossett LS, Jacobs JJ, Rubash HE. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res. 1998;356:144–153. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
