

Early diagnosis is associated with improved clinical outcomes in benign esophageal perforation: an individual patient data meta-analysis
- PMID: 32681374
- PMCID: PMC8195755
- DOI: 10.1007/s00464-020-07806-y
Early diagnosis is associated with improved clinical outcomes in benign esophageal perforation: an individual patient data meta-analysis
Abstract
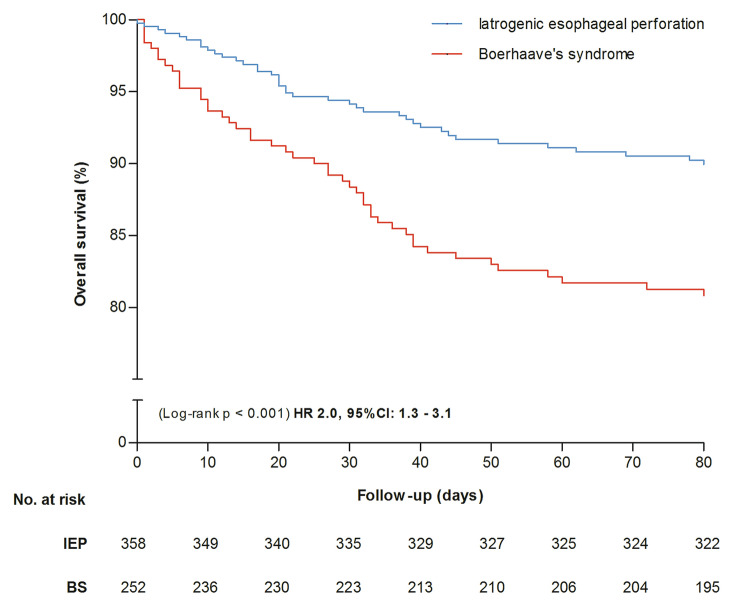
Background: Time of diagnosis (TOD) of benign esophageal perforation is regarded as an important risk factor for clinical outcome, although convincing evidence is lacking. The aim of this study is to assess whether time between onset of perforation and diagnosis is associated with clinical outcome in patients with iatrogenic esophageal perforation (IEP) and Boerhaave's syndrome (BS).
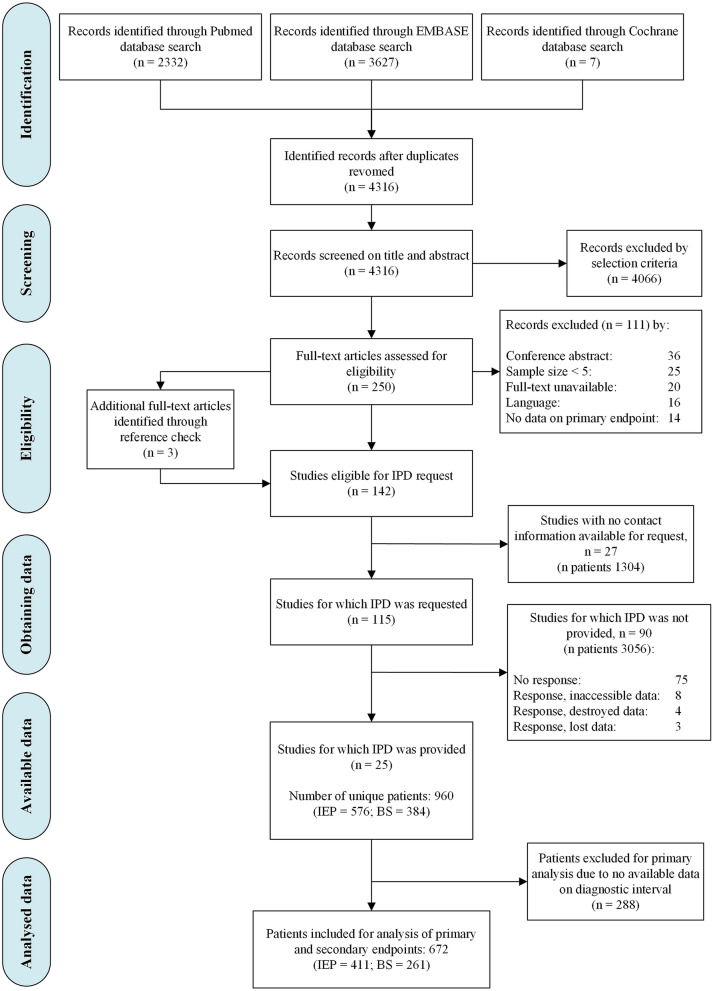
Methods: We searched MEDLINE, Embase and Cochrane library through June 2018 to identify studies. Authors were invited to share individual patient data and a meta-analysis was performed (PROSPERO: CRD42018093473). Patients were subdivided in early (≤ 24 h) and late (> 24 h) TOD and compared with mixed effects multivariable analysis while adjusting age, gender, location of perforation, initial treatment and center. Primary outcome was overall mortality. Secondary outcomes were length of hospital stay, re-interventions and ICU admission.
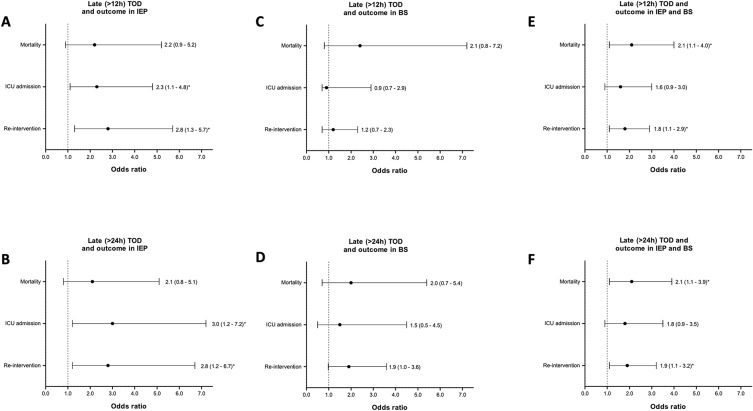
Results: Our meta-analysis included IPD of 25 studies including 576 patients with IEP and 384 with BS. In IEP, early TOD was not associated with overall mortality (8% vs. 13%, OR 2.1, 95% CI 0.8-5.1), but was associated with a 23% decrease in ICU admissions (46% vs. 69%, OR 3.0, 95% CI 1.2-7.2), a 22% decrease in re-interventions (23% vs. 45%, OR 2.8, 95% CI 1.2-6.7) and a 36% decrease in length of hospital stay (14 vs. 22 days, p < 0.001), compared with late TOD. In BS, no associations between TOD and outcomes were found. When combining IEP and BS, early TOD was associated with a 6% decrease in overall mortality (10% vs. 16%, OR 2.1, 95% CI 1.1-3.9), a 19% decrease in re-interventions (26% vs. 45%, OR 1.9, 95% CI 1.1-3.2) and a 35% decrease in mean length of hospital stay (16 vs. 22 days, p = 0.001), compared with late TOD.
Conclusions: This individual patient data meta-analysis confirms the general opinion that an early (≤ 24 h) compared to a late diagnosis (> 24 h) in benign esophageal perforations, particularly in IEP, is associated with improved clinical outcome.
Keywords: Esophageal rupture; Individual patient data meta-analysis; Time of diagnosis.
Conflict of interest statement
Peter D. Siersema declares that he currently receives research support from EllaCS (Czech Republic) and Pentax (Japan). He previously received research support from Boston Scientific (US), Cook Medical (Ireland) and EndoStim (US/The Netherlands). Manon C.W. Spaander declares that she has received research grants from Boston Scientific and Pyromed. Jon A. Tsai declares that he is an employee of Sanofi Genzyme. Bram D. Vermeulen, Britt van der Leeden, Jawad T. Ali, Tomas Gudbjartsson, Michael Hermansson, Donald E. Low, Douglas G. Adler, Abraham J. Botha, Xavier B. D’Journo, Atila Eroglu, Lorenzo E. Ferri, Christoph Gubler, Jan Willem Haveman, Lileswar Kaman, Richard A. Kozarek, Simon Law, Gunnar Loske, Joerg Lindenmann, Jung-Hoon Park, J. David Richardson, Paulina Salminen, Ho-Yong Song, Jon A. Søreide, Jeffrey N. Tarascio, Tim Vanuytsel, Camiel Rosman declares they have no conflict of interest.
Figures
References
-
- Ryom P, et al. Aetiology, treatment and mortality after oesophageal perforation in Denmark. Dan Med Bul. 2011;58(5):1–4. - PubMed
