The Wenckebach Phenomenon
- PMID: 32682381
- PMCID: PMC8142363
- DOI: 10.2174/1573403X16666200719022142
The Wenckebach Phenomenon
Abstract
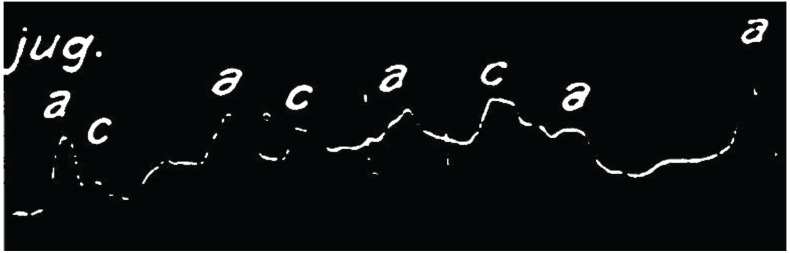
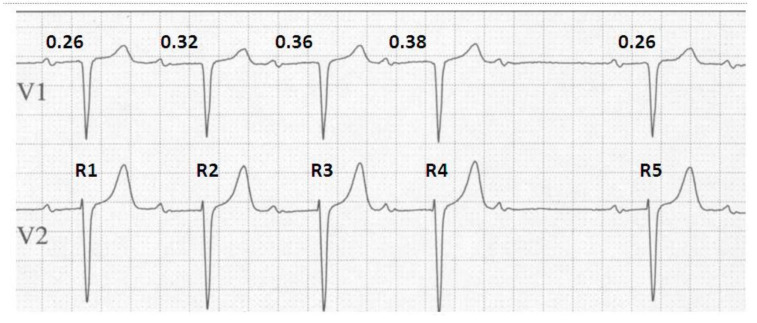
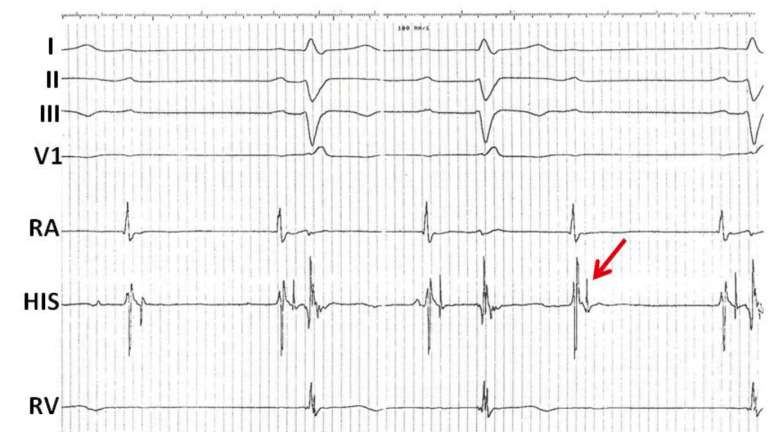
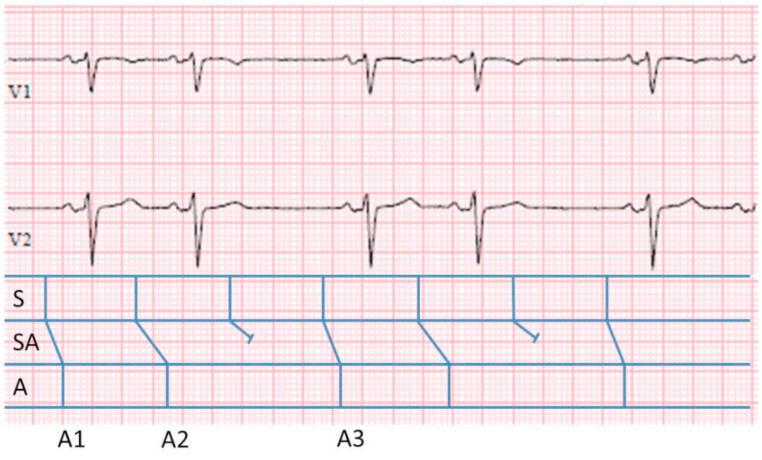
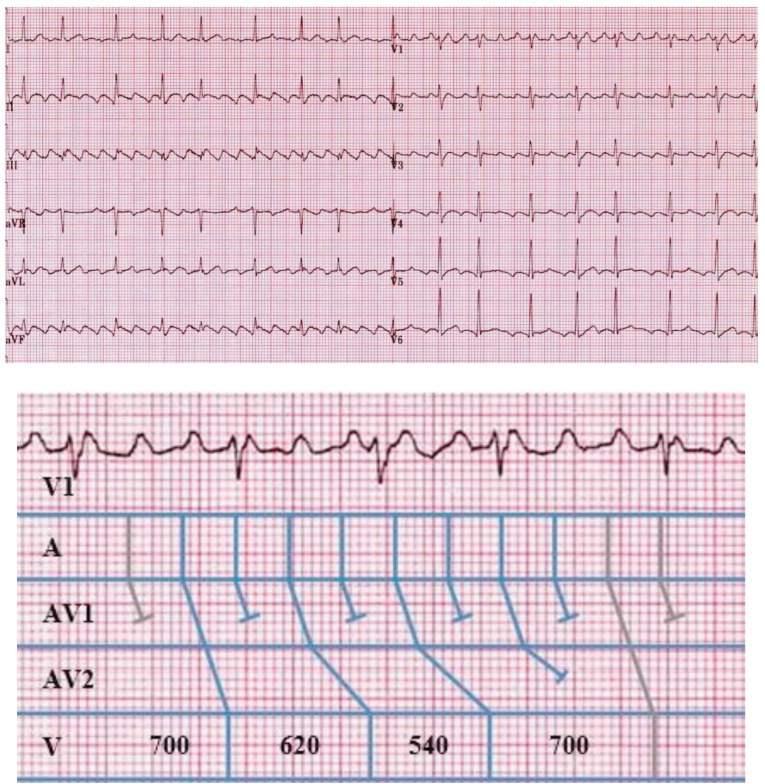
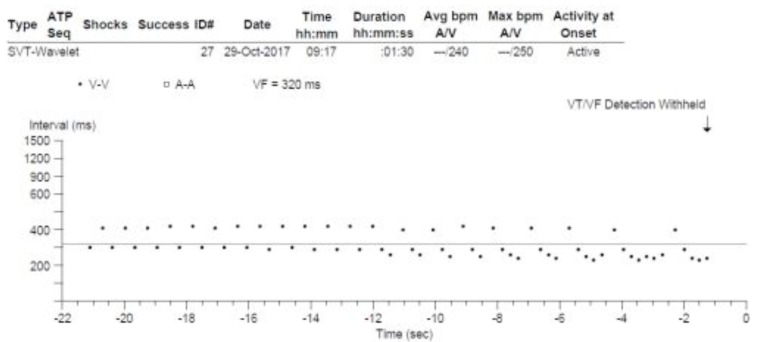
Medicine has many great pioneers, and in 1899, one such pioneer - Karel Frederik Wenckebach made a discovery which, even to this day, remains one of the fundamental concepts within electrophysiology. Since the Wenckebach Phenomenon was first described, the field of electrophysiology has developed at a rapid pace, allowing us to observe this behaviour, and its complexities, in many new ways. In a similar way, this chapter will illustrate Wenckebach behaviour across a spectrum of modalities from the 12 lead ECG, through to the intra-cardiac recordings from both electrophysiological studies and implantable cardiac devices. In doing so, we continue to shed light on the phenomenon first identified through Wenckebach's meticulous attention to detail some 120 years ago.
Keywords: AV node; ECG; Mobitz type 1; Wenckebach; atrioventricular block; electrophysiology.
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.net.
Figures
References
-
- Pérez-Riera A.R., Femenía F., McIntyre W.F., Baranchuk A. Karel Frederick Wenckebach (1864-1940): a giant of medicine. Cardiol. J. 2011;18(3):337–339. - PubMed
-
- Wenckebach K.F. On the analysis of irregular pulses. Z. Klin. Med. 1899;37:475–488.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources