

A multimodal intervention to improve hand hygiene compliance in peripheral wards of a tertiary care university centre: a cluster randomised controlled trial
- PMID: 32682429
- PMCID: PMC7368705
- DOI: 10.1186/s13756-020-00776-9
A multimodal intervention to improve hand hygiene compliance in peripheral wards of a tertiary care university centre: a cluster randomised controlled trial
Abstract
Background: Interventions to improve hand hygiene (HH) compliance are a key element in the practice infection prevention and control. It was our objective to assess the effect of a multimodal intervention on HH compliance at a tertiary care university hospital. As a secondary objective, we investigated the effect of the intervention on the occurrence of device-associated bloodstream infections.
Methods: We performed a single centre cluster randomised controlled trial at a university hospital in Germany. Twenty peripheral wards were invited to participate and randomly assigned to either the intervention (n = 10) or control group (n = 10). Quarterly, specifically trained student employees conducted direct compliance observations in all twenty wards. The intervention entailed dissemination of teaching materials on aseptic procedures, equipment with flexibly mountable alcoholic hand rub dispensers, and quarterly feedback on HH compliance.
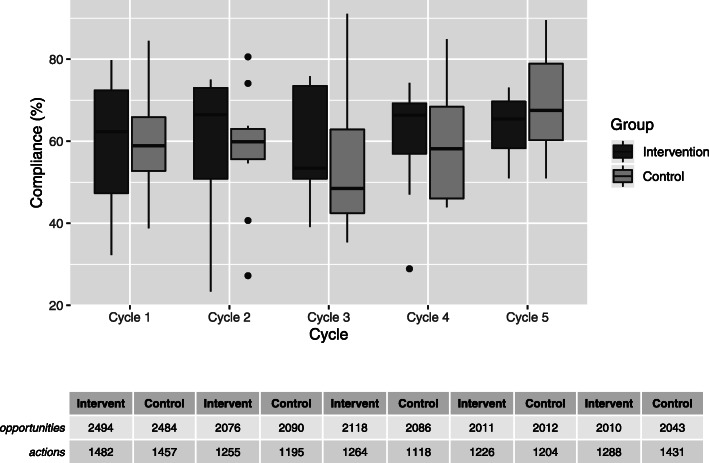
Results: In total, 21,424 HH opportunities were observed. Overall, compliance did not change significantly in either group (intervention group: 59% vs. 61% (1482 HH actions for 2494 HH opportunities vs. 5033 HH actions for 8215 HH opportunities), odds ratio (OR) 1.08 (95% confidence interval (CI95) 0.88, 1.33)); control group: 59% vs. 60% (1457 HH actions for 2484 HH opportunities vs. 4948 HH actions for 8231 HH opportunities), OR 1.06 (CI95 0.84, 1.35)). Compliance prior to aseptic procedures improved significantly in the intervention group from 44% (168 HH actions for 380 HH opportunities) to 53% (764 HH actions for 1452 HH opportunities) (OR 1.40 (CI95 1.04, 1.89), p = 0.03), while no significant increase was noted in the control group. In the intervention group, significantly fewer device-associated bloodstream infections per 1000 patient-days occurred than in the control group (84 vs. 123, incidence rate ratio 0.61 (CI95 0.46, 0.81), p < 0.01).
Conclusions: The lack of a significant overall improvement of HH compliance demonstrated that comprehensive implementation of HH interventions in multiple wards simultaneously is difficult. However, through targeted intervention measures, we were able to significantly increase HH compliance before aseptic procedures.
Keywords: Hand hygiene; Infection prevention; Multimodal intervention; Non-intensive care ward; Randomised controlled trial.
Conflict of interest statement
This trial was investigator initiated. BODE Chemie GmbH, a company of the HARTMANN group, funded the trial. S. Aghdassi, C. Schröder, E. Lemke, M. Behnke, P. Gastmeier and T. Kramer declare no further conflicts of interest. C. Plotzki and J. Wenk are employees of BODE Chemie GmbH. Throughout the study, P. Fliss was an employee of BODE Chemie GmbH.
Figures
References
-
- Grayson ML, Stewardson AJ, Russo PL, Ryan KE, Olsen KL, Havers SM, et al. Effects of the Australian National Hand Hygiene Initiative after 8 years on infection control practices, health-care worker education, and clinical outcomes: a longitudinal study. Lancet Infect Dis. 2018;18:1269–1277. doi: 10.1016/S1473-3099(18)30491-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
