

Characterization of a multicenter pediatric-hydrocephalus shunt biobank
- PMID: 32682437
- PMCID: PMC7368709
- DOI: 10.1186/s12987-020-00211-6
Characterization of a multicenter pediatric-hydrocephalus shunt biobank
Abstract
Background: Pediatric hydrocephalus is a devastating and costly disease. The mainstay of treatment is still surgical shunting of cerebrospinal fluid (CSF). These shunts fail at a high rate and impose a significant burden on patients, their families and society. The relationship between clinical decision making and shunt failure is poorly understood and multifaceted, but catheter occlusion remains the most frequent cause of shunt complications. In order to investigate factors that affect shunt failure, we have established the Wayne State University (WSU) shunt biobank.
Methods: To date, four hospital centers have contributed various components of failed shunts and CSF from patients diagnosed with hydrocephalus before adulthood. The hardware samples are transported in paraformaldehyde and transferred to phosphate-buffered saline with sodium azide upon deposit into the biobank. Once in the bank, they are then available for study. Informed consent is obtained by the local center before corresponding clinical data are entered into a REDCap database. Data such as hydrocephalus etiology and details of shunt revision history. All data are entered under a coded identifier.
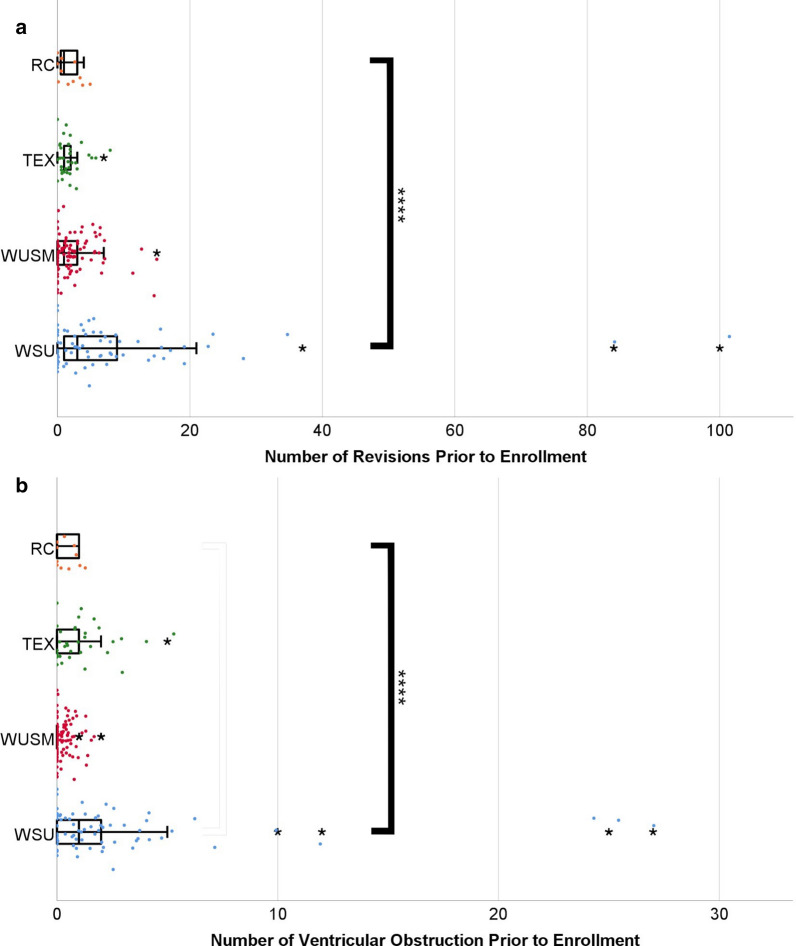
Results: 293 shunt samples were collected from 228 pediatric patients starting from May 2015 to September 2019. We saw a significant difference in the number of revisions per patient between centers (Kruskal-Wallis H test, p value < 0.001). The leading etiology at all centers was post-hemorrhagic hydrocephalus, a fisher's exact test showed there to be statistically significant differences in etiology between center (p = 0.01). Regression showed age (p < 0.01), race (p = 0.038) and hospital-center (p < 0.001) to explain significant variance in the number of revisions. Our model accounted for 31.9% of the variance in revisions. Generalized linear modeling showed hydrocephalus etiology (p < 0.001), age (p < 0.001), weight and physician (p < 0.001) to impact the number of ventricular obstructions.
Conclusion: The retrospective analysis identified that differences exist between currently enrolled centers, although further work is needed before clinically actionable recommendations can be made. Moreover, the variables collected from this chart review explain a meaningful amount of variance in the number of revision surgeries. Future work will expand on the contribution of different site-specific and patient-specific factors to identify potential cause and effect relationships.
Keywords: Biobank; CSF = cerebrospinal fluid; Hydrocephalus; Improving surgical outcomes; Multicenter; Retrospective cohort; Shunt failure; Shunt obstruction; Translational; Ventriculoperitoneal shunt.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Isaacs AM, Riva-Cambrin J, Yavin D, et al. Age-specific global epidemiology of hydrocephalus: systematic review, metanalysis and global birth surveillance [published correction appears in PLoS ONE. 2019 Jan 10;14(1):e0210851]. PLoS ONE. 2018;13(10):e0204926. Published 2018 Oct 1. 10.1371/journal.pone.0204926. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
